Month: February 2026
Male Fertility in 2026: The Overlooked Factor in IVF Success Rates
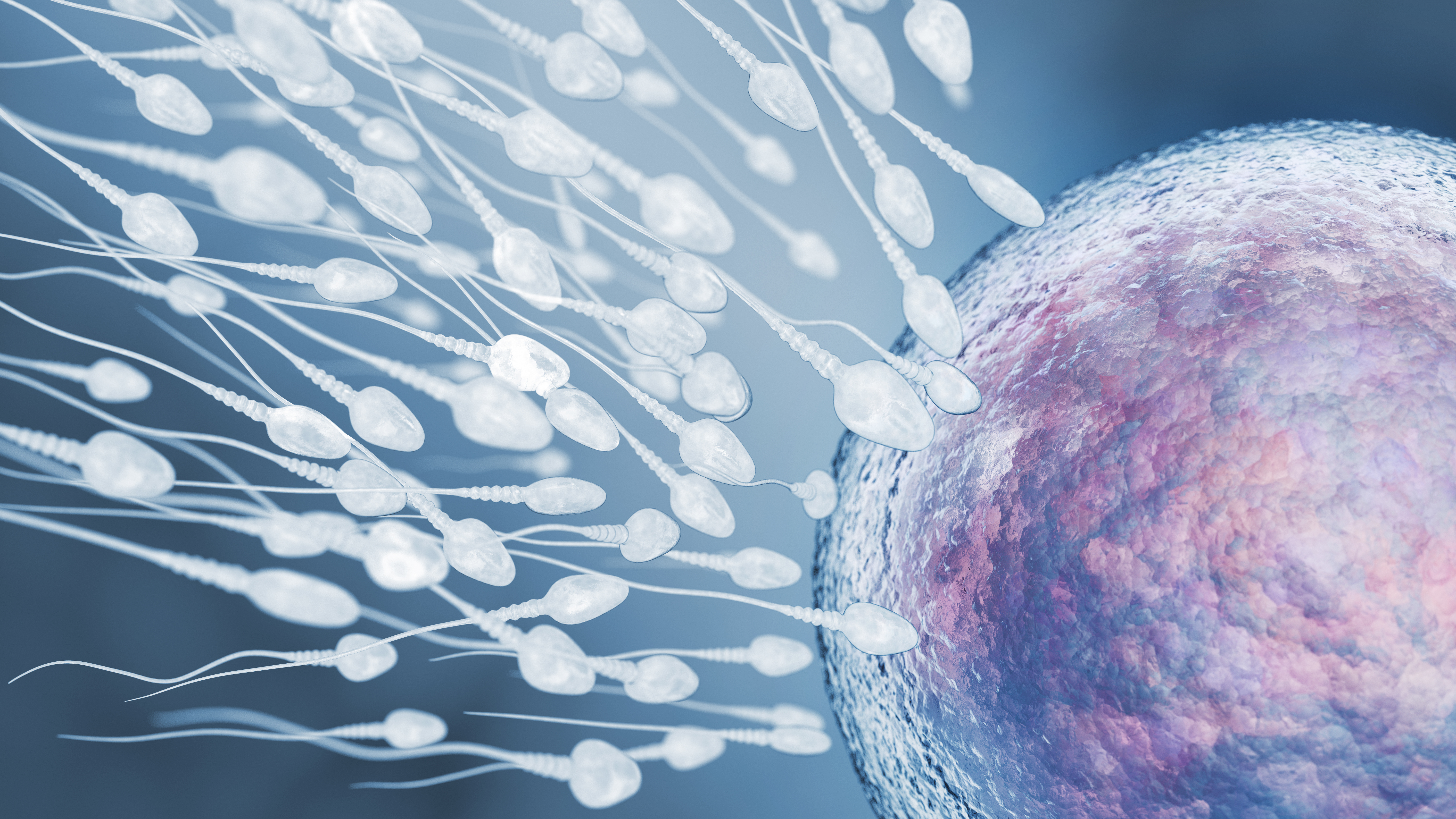
Male Fertility in 2026: The Overlooked Factor in IVF Success Rates
When couples begin IVF, the focus often lands on ovarian reserve, egg quality, and maternal age.
But in 2026, one fact remains consistently under-discussed:
Male factor contributes to nearly half of infertility cases.
Not partially.
Not occasionally.
Nearly half.
And yet, fertility conversations still default to women’s biology.
If you are navigating IVF, understanding male fertility data is not optional — it is foundational.
In Short
Male factor infertility contributes to approximately 40–50% of infertility cases. Sperm quality affects fertilization rates, embryo development, miscarriage risk, and IVF outcomes. In 2026, advanced testing such as sperm DNA fragmentation analysis is increasingly used, but lifestyle, age, and environmental exposure remain significant variables.
The Data Behind Male Fertility Decline
Over the past two decades, global research has documented a measurable decline in sperm concentration and total sperm count in many regions.
While causes remain multifactorial, contributors include:
• Environmental endocrine disruptors
• Obesity and metabolic syndrome
• Chronic stress
• Delayed fatherhood
• Sedentary lifestyle
• Smoking and alcohol us
Sperm is not static biology.
It reflects overall health.
What “Male Factor” Actually Means
Male factor infertility includes:
• Low sperm count (oligospermia)
• Poor motility (asthenozoospermia)
• Abnormal morphology
• High sperm DNA fragmentation
• Obstructive causes
• Hormonal imbalance
Even when semen analysis appears “normal,” subtle sperm DNA damage may affect embryo development.
This is where deeper testing sometimes becomes relevant.
Join Sistapedia®
Trying to understand how sperm quality affects your IVF plan?
Join Sistapedia for clear, evidence-based reproductive health guidance built for real decisions.
Sperm Quality and IVF Outcomes
Sperm influences:
• Fertilization success
• Embryo cleavage timing
• Blastocyst quality
• Miscarriage risk
Even with ICSI (intracytoplasmic sperm injection), where a single sperm is injected into an egg, sperm DNA integrity still matters.
ICSI bypasses motility issues.
It does not repair DNA fragmentation.
Sperm DNA Fragmentation: What It Means
DNA fragmentation refers to breaks or damage in sperm genetic material.
High fragmentation has been associated with:
• Lower implantation rates
• Higher miscarriage rates
• Reduced embryo quality
However, routine DNA fragmentation testing is still debated in first-cycle IVF patients.
It is more often considered in:
• Recurrent miscarriage
• Repeated IVF failure
• Unexplained infertility
As with many fertility tools, context matters.
Male Age and Fertility
While female age dominates reproductive discussions, male age is not irrelevant
Advanced paternal age has been associated with:
• Increased DNA fragmentation
• Slightly increased miscarriage risk
• Increased risk of certain genetic conditions
Sperm production continues across life — but quality shifts over time.
Lifestyle Impact on Sperm Health
Unlike egg reserve, sperm production renews approximately every 70–90 days.
That means:
• Dietary changes
• Exercise
• Reduced alcohol intake
• Smoking cessation
• Stress management
can influence sperm parameters within months.
This creates an opportunity.
Male fertility is not entirely fixed.
Share Your Story
Has male factor played a role in your IVF journey?
Share your experience on Sistapedia® and apply for your Pink Tick. Your insight helps normalize conversations that are too often avoided.
When to Test Further
Discuss additional testing with your doctor if:
• IVF fertilization rates were unexpectedly low
• There is recurrent miscarriage
• There are repeated implantation failures
• Semen analysis shows borderline results
• The male partner is over 40 with no prior evaluation
Ask:
• Would DNA fragmentation testing change management?
• Would antioxidant therapy or lifestyle change be recommended?
• Does this influence embryo selection decisions?
Avoid testing that does not alter treatment.
The Emotional Layer
Male infertility often carries stigma.
Silence.
Shame.
Avoidance.
But fertility is shared biology.
Blame has no place in medical reality.
Couples navigating IVF deserve balanced assessment from the beginning.
Frequently Asked Questions
How common is male infertility?
Male factor contributes to roughly 40–50% of infertility cases.
Can poor sperm quality affect IVF success?
Yes. It can influence fertilization rates, embryo development, and miscarriage risk.
Does ICSI solve male infertility?
ICSI bypasses motility and count issues but does not correct sperm DNA damage.
Can sperm quality improve?
In some cases, yes. Lifestyle changes may influence sperm parameters over several months.
The Bigger Picture
IVF conversations often begin with ovarian reserve numbers.
But successful fertility care requires full evaluation — not assumptions.
In 2026, the strongest fertility outcomes occur when:
Both partners are assessed early.
Data guides decisions.
Stigma is removed from male testing.
Fertility is not a female issue.
It is a shared biological equation.
Join Sistapedia® for trusted reproductive health education grounded in clarity.
Share your IVF journey and become a Pink Tick Sista — your experience may help another couple start the right conversation sooner.
Fertility specialists and clinics committed to balanced evaluation: Apply for Crown Verification and connect with patients seeking transparent care.
IVF Success Rates in 2026: What Clinics Don’t Always Explain About Your Chances

When you sit in a fertility clinic, one number can shape everything.
“Your success rate is 42%.”
It sounds precise. Scientific. Reassuring — or devastating.
But what does that number actually mean?
In 2026, IVF success rates are widely published, compared online, and used to market clinics. Yet many patients still misunderstand what those percentages represent — and what they don’t.
Let’s break it down clearly.
In Short
IVF success rates are usually reported as live birth rates per cycle or per embryo transfer. They vary significantly by age, diagnosis, and clinic practices. A reported percentage does not guarantee outcome, and cumulative success over multiple cycles is often higher than a single-cycle statistic suggests.
What “IVF Success Rate” Actually Measures
The most meaningful statistic is:
Live birth rate per embryo transfer.
Not:
• Positive pregnancy test rate
• Implantation rate
• Clinical pregnancy rate
Only live birth reflects the outcome most patients care about.
However, clinics may publish different numbers:
• Live birth per cycle started
• Live birth per retrieval
• Live birth per transfer
• Cumulative live birth across multiple cycles
Each tells a slightly different story.
IVF Live Birth Rates by Age (2026 Averages)
While numbers vary by country and clinic, broad registry data suggests:
• Under 35: ~45–55% per transfer
• 35–37: ~35–45%
• 38–40: ~20–30%
• 41+: ~10–20%
Age remains the single strongest predictor of IVF outcome.
No laboratory technology reverses ovarian aging.
Why Clinic Success Rates Differ
Not all clinics report the same way.
Some differences reflect genuine expertise. Others reflect patient selection.
For example:
• A clinic treating younger patients may show higher success rates.
• A clinic accepting more complex cases may show lower percentages.
• A clinic transferring multiple embryos may increase pregnancy rates — but also twin risk.
Success rates are not only about skill.
They reflect population.
Join Sistapedia®
Trying to interpret IVF statistics and feeling overwhelmed?
Join Sistapedia® for clear, evidence-based reproductive health guidance designed for women navigating real decisions.
Per Transfer vs Per Cycle: Why It Matters
Imagine this scenario:
You retrieve 10 eggs.
Three embryos develop.
Two transfers occur.
If the clinic reports per transfer, you might see:
“50% live birth rate.”
But if reported per cycle started, the number may be lower.
Both are technically correct. Context matters.
Cumulative Success Is Often Higher
Many patients focus on single-cycle percentages.
But cumulative live birth probability increases over multiple attempts.
For example:
If one cycle gives a 40% chance of live birth,
Two cycles do not simply double it to 80%.
Probability accumulates differently.
This is why doctors often discuss “three-cycle outlook” rather than one.
The emotional difficulty lies in uncertainty between cycles.
The Role of Embryo Quality
Success rates are strongly influenced by:
• Embryo quality
• Chromosomal normality
• Uterine environment
• Sperm parameters
Even with advanced grading systems and modern laboratory conditions, biology remains variable.
Two embryos with similar grades can lead to different outcomes.
When Statistics Become Marketing
In competitive fertility markets, success rates are a powerful marketing tool.
Important questions to ask:
• Are these live birth rates or pregnancy rates?
• Are donor egg cycles included?
• Is the data independently audited?
• Does this apply to my age group?
If a number sounds unusually high, request clarification.
Transparency should not be uncomfortable for a reputable clinic.
Share Your Story
Have you been quoted a success rate that felt confusing or misleading?
Share your IVF journey on Sistapedia and receive your Pink Tick. Your experience helps other women navigate the numbers with confidence.
Emotional Impact of Percentages
A 30% success rate can feel like:
• Hope
• Fear
• Pressure
• Urgency
But numbers are not predictions about your personal worth or outcome.
They reflect population averages.
IVF is medicine layered onto biology.
Even perfect conditions cannot eliminate uncertainty.
When to Speak With Your Doctor
Before beginning IVF — or before another cycle — ask:
• What is my live birth rate per transfer in my age group?
• What is the cumulative chance after three cycles?
• How many embryos do we expect based on my ovarian reserve?
• What is the miscarriage risk in my case?
• What factors could improve or reduce my outcome?
Clarity reduces anxiety.
Avoid vague reassurance. Seek specific explanation.
Frequently Asked Questions
Is IVF more successful now than 10 years ago?
Laboratory improvements and embryo culture advancements have increased consistency, but age remains the dominant factor.
Does using genetic testing improve IVF success rates?
Genetic testing may reduce miscarriage risk in certain age groups but does not universally increase cumulative live birth rates.
How many IVF cycles does the average person need?
Many women conceive within one to three cycles, but this varies by age and diagnosis.
Should I choose the clinic with the highest published success rate?
Ask how their data applies to your personal profile before deciding.
The Bigger Picture
In 2026, IVF statistics are easier to access than ever.
But access does not equal understanding.
The most informed patients are not those chasing the highest percentage.
They are the ones asking:
What does this mean for me?
IVF success rates are not promises.
They are probabilities.
And probability deserves explanation.
Join Sistapedia® for trusted reproductive health education grounded in clarity — not marketing.
Share your IVF experience and become a Pink Tick Sista. Your insight may help another woman interpret her numbers more confidently.
Fertility specialists and clinics committed to transparent reporting: Apply for Crown Verification and connect with women actively researching their options.
AI Fertility Scores in 2026: Are Predictive Algorithms Replacing Human Judgment?
If you’re undergoing IVF in 2026, there’s a high chance an algorithm is involved in your treatment plan.
Not just your doctor.
An algorithm.
Clinics are increasingly using AI fertility prediction models to estimate:
• Your probability of live birth
• Which embryos to transfer
• Whether to recommend add-ons
• Whether another cycle is “worth it”
But here’s the critical question:
Are these tools improving outcomes — or quietly reshaping decision-making without full transparency?
Quick Answer
AI fertility scores use machine learning models trained on large IVF datasets to predict live birth probability, embryo viability, and treatment outcomes. They can improve embryo selection accuracy but are not guarantees. Human clinical judgment remains essential, as AI tools depend on data quality, patient variables, and model bias.
What Is an AI Fertility Score?
An AI fertility score is a predictive output generated by machine learning systems trained on thousands (sometimes millions) of IVF cycles.
These systems analyze:
• Age
• AMH levels
• Antral follicle count
• Hormone response
• Embryo imaging data
• Sperm parameters
• Prior cycle outcomes
They generate a probability estimate — often expressed as:
“Estimated live birth probability: 48%”
This feels precise.
But precision is not certainty.
How Accurate Are AI Fertility Predictions?
Studies published between 2023–2025 show:
• AI-assisted embryo selection improves implantation prediction modestly (5–10% improvement in some clinics).
• Predictive models are strongest when trained on large, diverse datasets.
• Performance declines when applied to populations outside the training data.
In other words:
AI works best when you resemble the patients in its database.
This introduces bias risk.
Comparison: Human vs AI Embryo Selection
Factor Embryologist Judgment AI-Assisted Grading
Experience-based Yes No
Data-scale Limited to clinic Thousands+ cases
Fatigue Possible None
Bias Human cognitive bias Data bias
Adaptability High Depends on retraining
The future is not AI vs human.
It is AI + human.
Where AI Helps
AI shows promise in:
1. Time-lapse embryo imaging (morphokinetics)
2. Pattern detection invisible to human eyes
3. Risk prediction modeling
4. Large-scale outcome correlation
It reduces inter-observer variability between embryologists.
It standardizes grading.
That is valuable.
Where AI Falls Short
AI cannot:
• Measure emotional resilience
• Predict future uterine receptivity perfectly
• Account for sudden hormonal variability
• Replace shared decision-making
Most importantly:
AI models depend on historical data.
If fertility medicine evolves — AI must retrain.
The Ethical Question
Are patients fully informed when AI influences:
• Add-on recommendations?
• Cycle continuation decisions?
• Embryo discard vs transfer?
Transparency varies between clinics.
Women often receive a percentage — but not an explanation of how it was generated.
That’s a knowledge gap.
Sistapedia’s Free Pink Tick for Sista’s
Have you gone through IVF with AI-assisted grading or predictive dashboards?
Share your story on Sistapedia® and receive your free Pink Tick — your experience helps other women ask better questions.
IVF Add-Ons and Algorithmic Upselling
A growing concern in 2026:
AI recommendations may increase uptake of:
• PGT-A testing
• ERA testing
• Additional stimulation cycles
• Embryo banking
These may be medically justified — but financial incentives exist.
Women deserve clarity:
Is this recommendation statistically necessary — or probability-based optimization?
When to See a Doctor (Not Just Trust the Score)
Ask your reproductive endocrinologist:
• How is this AI model trained?
• What dataset does it use?
• Has it been validated in peer-reviewed studies?
• What is the model’s error margin?
• Does it change treatment recommendations — or just inform them?
If answers are vague, request clarification.
Sistapedia’s Crown Verification
Are you a reproductive endocrinologist or embryologist using AI tools?
Apply for Crown Verification on Sistapedia® and explain your methodology transparently to patients actively researching these technologies.
FAQ
Are AI fertility predictions accurate?
AI improves prediction modestly but does not guarantee live birth. Accuracy depends on dataset quality and patient similarity to training data.
Does AI choose which embryo to transfer?
AI assists in grading but final decisions should involve clinical judgment.
Is AI better than embryologists?
AI reduces variability and detects patterns, but human expertise remains essential.
Should I trust IVF success rate percentages from clinics?
Ask how the number was calculated and whether it includes AI modeling assumptions.
Final Perspective
AI fertility scores are tools.
Powerful tools.
But they are not destiny.
The strongest IVF outcomes in 2026 occur when:
Data informs decisions.
Doctors interpret context.
Patients understand probabilities.
That’s informed consent in the AI era.
Join Sistapedia® — free access to AI-verified reproductive health education.
Share your IVF journey and become a Pink Tick Sista — your experience may shape another woman’s questions.
Clinicians using AI tools: Apply for Crown Verification and lead transparent, ethical fertility practice in the AI age.
Fertility Investment Strategy: Is Egg Freezing Worth It in 2026?

Egg freezing used to be whispered about.
Now it’s marketed as empowerment.
But beneath the empowerment narrative is a harder question:
Is egg freezing actually worth it — medically, financially, and emotionally?
In 2026, women are freezing eggs later, spending more, and expecting clearer returns. It’s time to look at the numbers.
Quick Answer
Egg freezing can increase future reproductive options but does not guarantee a baby. Success depends heavily on age at freezing, number of eggs retrieved, and future IVF outcomes. Financially, costs range from $8,000–$20,000 per cycle plus storage, and multiple cycles may be needed. It is a risk management strategy, not fertility insurance.
The Medical Reality: What Egg Freezing Actually Does
Egg freezing (oocyte cryopreservation) preserves unfertilized eggs at a younger biological age.
It does NOT:
• Guarantee pregnancy
• Stop aging
• Eliminate IVF
• Remove miscarriage risk
In 2025–2026 data, live birth rates per frozen egg vary significantly by age:
Age at Freezing Estimated Live Birth Probability per 15–20 Eggs
Under 35 60–70% cumulative chance
35–37 40–55% cumulative chance
38–40 25–40% cumulative chance
41+ Below 15–20%
(Source: multi-center IVF registry analyses 2024–2025)
Age is the dominant variable.
The Financial Breakdown
Average cost per cycle (US/Australia comparable markets):
• Stimulation + retrieval: $8,000–$15,000
• Medications: $3,000–$6,000
• Storage annually: $500–$1,200
• Future IVF thaw cycle: $5,000–$10,000
Most women require 1–3 cycles to bank 15–25 eggs.
Total projected investment over time:
$15,000–$45,000+
This reframes egg freezing as a capital allocation decision, not just a medical procedure.
Sista Sign-Up
Want personalized guidance and trusted info? Join Sistapedia® — it’s free to sign up and built specifically for women navigating fertility decisions.
Is Egg Freezing a Financial Asset?
Some women view frozen eggs as:
• Career flexibility insurance
• Relationship timing buffer
• Psychological relief
• Optionality preservation
But unlike financial assets:
• Eggs depreciate biologically if frozen later
• Not all eggs survive thaw
• Not all fertilise
• Not all implant
It’s more accurate to call egg freezing a risk hedge rather than an investment.
Comparison: Freeze Eggs vs Try Naturally at 38+
Factor Freeze at 32 Try Naturally at 38
Egg Quality Higher Lower
IVF Likelihood Still likely Highly likely
Financial Cost High upfront Possibly higher later
Emotional Certainty Medium Low
Biological Risk Lower Higher
This is not a moral choice. It’s a probabilistic one.
Emotional ROI: The Hidden Variable
Many women report:
• Reduced anxiety after freezing
• Increased dating confidence
• Temporary relief
However, psychological literature suggests that perceived fertility security can create delay bias — a false sense of guaranteed outcome.
Egg freezing reduces uncertainty, but it does not eliminate it.
Sista’s Pink Tick
Have you frozen your eggs? Regret it? Glad you did?
Share your story on Sistapedia and get your free Pink Tick — our verified badge for Sistas who speak up and support others.
The Statistical Reality
In 2024 registry data:
• Roughly 50–60% of women who freeze eggs never return to use them.
• Of those who do, live birth rates depend primarily on age at freezing.
The procedure is safest under age 35. After 38, diminishing returns accelerate.
When to See a Doctor
You should consult a reproductive endocrinologist if:
• You are 32–37 and not planning pregnancy within 3–5 years.
• You have low AMH (Anti-Müllerian Hormone).
• You have family history of early menopause.
• You have PCOS, endometriosis, or diminished ovarian reserve.
• You are considering delaying childbearing beyond 38.
Clinical terminology to understand:
• Diminished ovarian reserve (DOR)
• Oocyte cryopreservation
• Controlled ovarian hyperstimulation
• Live birth rate per thaw cycle
Experts, Medical Doctors, (MD’s) Registered Nurses,( RN’s), Healthcare Practitioners (HCP’s), – Crown Verification
If you’re a fertility specialist, reproductive endocrinologist, or clinic, become a Crown Verified expert on Sistapedia and be discoverable to women making high-stakes decisions.
FAQ
Is egg freezing worth it financially in 2026?
It depends on age, income, and risk tolerance. For women under 35, it may provide meaningful reproductive optionality. After 38, cost-to-success ratios decline sharply.
How many eggs should I freeze to have one baby?
Most specialists recommend 15–20 mature eggs under age 35 to optimize cumulative live birth probability.
Does egg freezing guarantee pregnancy later?
No. Egg survival, fertilization, embryo development, and implantation all impact outcomes.
Is egg freezing safer now than 10 years ago?
Yes. Vitrification techniques have improved survival rates, but success still depends heavily on age.
Final Reality Check
Egg freezing is not a panic move.
It is not a feminist badge.
It is not a guarantee.
It is a strategic option — best used early, with clear expectations, and under expert guidance.
Join Sistapedia® today — free sign-up for trusted, AI-verified reproductive health guidance.
Share your fertility story and become a Pink Tick Sista — your voice may help another woman decide sooner.
Clinicians and fertility experts: apply for Crown Verification and connect with women actively researching egg freezing decisions.
The Unpaid Reproductive Labour Propping Up Modern Economies

Unpaid Reproductive Labour
Governments obsess over:
• GDP
• Productivity
• Skills shortages
• Falling birth rates
What they mostly ignore is the foundation all of this stands on:
The unpaid reproductive labour — mostly done by women — that produces, raises and maintains the humans who keep economies running.
This isn’t just “motherhood” in the sentimental sense.
It’s the hard, unglamorous work of:
• Planning and preventing pregnancies
• Going through fertility treatment and losses
• Pregnancy, birth and postpartum recovery
• Feeding and night care
• Managing children’s health, schooling and therapy
• Caring for ageing parents and sick relatives
• Running the medical and emotional admin for entire families
Modern economies assume this labour will just happen, reliably and for free — like oxygen.
This article breaks down:
• What unpaid reproductive labour actually includes
• How it silently subsidizes GDP, corporate profits and public budgets
• The health and financial cost to the women doing it
• Why naming and valuing this labour matters for policy, workplaces and women’s lives
• Where Sistapedia® sits in this picture
What Counts as “Unpaid Reproductive Labour”?
Reproductive labour = work that creates, sustains and cares for human beings so they can participate in society and the economy.
When it’s unpaid, it disappears from the stats but not from women’s bodies.
1. Biological and Clinical Work
• Managing contraception and side-effects
• Tracking cycles, appointments and tests for fertility treatment
• Pregnancy: nausea, fatigue, pain, scans, monitoring, risk management
• Labour and birth: vaginal, instrumental, caesarean, complications
• Miscarriage, ectopic pregnancy, termination, stillbirth — plus physical and emotional recovery
• Postpartum recovery: bleeding, wound healing, pelvic floor issues, mental health
None of this is “just nature.” It’s intense physical and psychological labour.
2. Infant Feeding and Early Care
• Breastfeeding (latching struggles, pain, mastitis, pumping logistics)
• Bottle-feeding (sterilising, mixing, cleaning, night feeds)
• Settling and soothing, night wakes, sleep deprivation
• Monitoring growth, development, rashes, fevers, feeding issues
If you costed breastfeeding alone as paid labour (training, time, night work, wear and tear on the body), it wouldn’t be a soft-focus lifestyle choice. It would look like a demanding shift job.
3. Ongoing Childcare and Development Work
• Dressing, feeding, bathing, supervising
• School runs, daycare drop-offs and pick-ups
• Homework support and school projects
• Emotional regulation: meltdowns, worries, friendship dramas
• Behavioral support and boundaries
This is the daily production of future workers and taxpayers — treated as “just parenting.”
4. Health & Education Admin (The “Invisible” Layer)
• Booking and tracking GP, specialist, dental, therapy appointments
• Tracking medications, scripts, test results
• Reading and responding to school emails, forms and portals
• Organizing uniforms, equipment, lunches, excursions, sports, performances
Most of this planning and tracking lives in one person’s head. In most households, that person is a woman.
5. Extended Care
• Caring for elderly parents and relatives
• Managing their appointments, medications, finances and crises
• Supporting partners through illness, job loss, stress or burnout
This is reproductive labour too: sustaining human beings who are no longer “economically productive” but still very much alive and dependent.
If We Priced It, Economies Would Look Very Different
National time-use surveys and economic studies vary by country and method, but they keep landing on the same headline:
If unpaid care and domestic work were counted, it would represent a huge share of economic activity — often equivalent to a double-digit percentage of GDP.
Common patterns across those studies:
• Women consistently do more hours of unpaid care and domestic work than men — often 2–3× as much, even in dual-income households.
• When you apply a market replacement rate (what you’d pay workers to do this care), the value runs into trillions globally.
• In some countries, estimates of unpaid work’s value reach 20–40%+ of measured GDP depending on methodology.
You don’t need exact decimal points to see the structural reality:
• Governments, employers and markets are being heavily subsidized by unpaid reproductive labour.
• If they had to pay full price for it, profits, budgets and growth projections would look very different.
How Unpaid Reproductive Labour Subsidizes Everything Else
1. It Subsidizes the workforce
Every “productive” worker:
• The nurse on night shift
• The software engineer
• The teacher, warehouse worker, clinic receptionist
• The researcher, cleaner, CEO
…exists because, at some point, someone:
• Carried them, birthed them and recovered
• Kept them alive, fed and cared for
• Took them to doctors, schools, therapists
• Managed sickness, behavior, paperwork and logistics
In most cases, that “someone” has been a woman doing unpaid or underpaid labour.
When we talk about a “skilled workforce” or “human capital,” we’re talking about people produced and maintained by reproductive labour that rarely gets recognized, let alone compensated.
2. It Subsidizes Tomorrow’s GDP
Policymakers worry about:
• Declining fertility
• Ageing populations
• “Not enough young workers”
But they often treat childbirth and childrearing like a natural resource that will keep flowing — instead of a high-risk, high-cost process mostly carried by women.
The state and the market want:
• Enough babies born
• Enough children raised, educated and healthy
• Enough future taxpayers and workers
They do not fully carry the cost of:
• Fertility treatment when conception isn’t straightforward
• Pregnancy risk, birth trauma and long-term impacts
• Postpartum recovery and mental health care
• Years of unpaid childcare, health admin and education support
Those costs are internalized by families — usually women — and written out of the national accounts.
3. It Subsidizes Health and Education Systems
Health and education systems quietly depend on unpaid reproductive labour to function.
For health:
• Women monitor symptoms, follow up results, chase referrals
• They take time off work to attend appointments — their own, their children’s, their parents’
• They provide day-to-day care around surgeries, hospitalizations and chronic conditions
For education:
• Parents (usually mothers) read the emails, respond to forms, handle payments
• They help with homework, projects, behavior and mental health
• They arrange diagnostics, therapy, tutoring and adjustments when needed
If all of that invisible work stopped, hospitals, clinics and schools would be overwhelmed almost immediately.
The Health Cost to the Women Doing It
Unpaid reproductive labour isn’t just an economic issue. It’s a health crisis hiding in plain sight.
Common consequences:
• Chronic sleep deprivation: fragmented nights with babies, young kids, teens, or ageing parents
• Delayed or dismissed care for women themselves:
• Endometriosis, adenomyosis, heavy bleeding
• PCOS, thyroid issues, autoimmune disease
• Perinatal depression and anxiety
• Perimenopause and menopause symptoms
• Mental health strain:
• Anxiety from constant responsibility
• Depression and burnout
• Trauma from birth complications, NICU stays, loss
The standard response women hear is:
• “You need to prioritise self-care.”
• “Try stress management.”
• “Maybe it’s just anxiety.”
But telling women to “self-care” while leaving their structural load unchanged is like telling someone carrying a 100-kg backpack to “work on their posture.”
Why the Market Doesn’t Self-Correct
If this work is so valuable, why doesn’t the market pay for it automatically?
Because of structural factors:
1. You can’t outsource all of it
• You can hire childcare; you can’t outsource pregnancy.
• You can hire support workers; you can’t outsource being the legally responsible parent or next of kin.
2. The benefits are spread out
• The gains from reproductive labour go to:
• Children themselves
• Employers (present and future)
• Governments via taxes
• Partners, extended family and communities
• No single actor feels responsible for paying full cost.
3. It’s coded as love, not labour
• “You do it because you love your family.”
• Asking for money, time or structural support is framed as selfish or ungrateful.
4. Workplaces are still designed around an “unencumbered worker”
• Historically, that worker had a full-time, unpaid carer in the background (a wife or mother).
• Even with dual-income households, many workplace expectations haven’t adjusted.
Result: the system free-rides on women’s unpaid labour and then labels them “unproductive” if they step back or burn out.
Why Naming This Matters
When unpaid reproductive labour is invisible:
• Women blame themselves for being tired, scattered, unwell or “not resilient enough.”
• Policy focuses on “getting more women into work” without counting the work they already do.
• Healthcare treats burnout, pain and mood as individual pathology instead of structural overload.
Naming it as reproductive labour does three things:
1. Shifts blame off individual women
• You’re not failing at life; you’re carrying a load designed for multiple people, unpaid.
2. Creates leverage for policy and workplace change
• If governments and employers depend on this labour, they should share its costs and risks.
3. Justifies building new systems and platforms around women’s realities
• Tech, healthcare and community infrastructure can be redesigned to work with, not against, the load women carry.
How Sistapedia Fits Into This Picture
Sistapedia is being built precisely because women’s unpaid reproductive labour and health have been treated as background noise.
Sistapedia® is:
• An AI-verified marketplace and social platform dedicated to women’s reproductive health across the lifecycle:
• Periods, contraception, endometriosis, PCOS
• Fertility, IVF, pregnancy, birth, postpartum
• Breastfeeding, parenting, perimenopause, menopause
The aim:
• Not to romanticize unpaid labour
• But to centre the women doing it and give them tools, information, verification and pathways to economic participation tied to their expertise and experience
For Sista’s
Every time you:
• Explain what IVF actually feels like
• Share how endometriosis affects your work and family life
• Talk honestly about breastfeeding, sleep deprivation, birth trauma or perimenopause
• Support other women in making decisions about clinics, products, treatments
…you are performing high-value reproductive labour that others — from brands to clinics to policymakers — benefit from.
On Sistapedia®, you’ll be able to:
• Build a profile that recognizes your lived experience with our Pink Tick identity verification for Sista’s
• Participate in a community where your knowledge is treated as an asset, not a side note
• Be part of an ecosystem explicitly designed around women’s reproductive health, not generic “wellness” content
For Experts, Clinicians, Products & Brands
If you work in:
• Fertility, IVF, obstetrics, gynecology
• Menstrual, hormonal, pregnancy or menopause care
• Mental health linked to reproductive life stages
• Products and services in women’s health
You already operate in a system propped up by women’s unpaid labour:
• Self-education
• Peer support
• Informal product testing and recommendation
• Health and admin work around your services
Sistapedia’s verification model (Crown tiers for professionals, experts, clinics, products & brands) is built to:
• Make trust more transparent and accountable
• Connect Sistas with verified options in a category full of noise and misinformation
• Acknowledge that women’s lived experience and professional expertise are both critical parts of the infrastructure
What Needs to Change Beyond Any One Platform
Recognizing unpaid reproductive labour isn’t enough; it needs to feed into real changes:
1. Measurement in official statistics
• Time-use surveys integrated into economic planning
• Regular valuation of unpaid care and reproductive labour
2. Social and health policy
• Paid parental leave that actually supports recovery and bonding
• Accessible, affordable childcare
• Serious investment in reproductive health (endo, PCOS, miscarriage, fertility, menopause)
3. Legal and financial recognition in families
• Property and asset division that accounts for unpaid care roles
• Superannuation/pension protections for time spent out of paid work caring
4. Workplace design and culture
• Genuine flexibility that doesn’t quietly punish women’s careers
• Support for fertility treatment, pregnancy, postpartum, perimenopause and caregiving
• Clear policies so women aren’t forced to “wing it” or hide what they’re carrying
Sistapedia® is one part of that bigger shift: a dedicated environment where women’s reproductive labour and health are treated as central infrastructure, not a special interest.
Final Word: You’re Not “Just Helping Out” — You’re Holding Up the System
If you’ve ever said:
• “I’m just at home with the kids.”
• “I just do the appointments and school stuff.”
• “I just look after Mum/Dad when they’re unwell.”
Start translating that accurately:
• “I perform unpaid reproductive labour that keeps multiple humans — and by extension, the economy — functioning.”
You shouldn’t have to be heroic, silent or sick to make that visible.
Platforms like Sistapedia®, better policy, and more honest workplace design are all part of the same correction:
• Stopping the free-ride on women’s bodies and time
• Naming reproductive labour as real work
• Building systems that finally treat you as infrastructure, not background
You are not an accessory to the economy.
You are part of the machinery that makes it possible.
You’re Not Bad at Rest — You’re Never Actually Off Duty

Women Mental Load Rest
You sit down on the couch “to rest.”
Five minutes later, your brain is:
• Replaying a conversation from this morning
• Running through three different to-do lists
• Wondering what’s for dinner tomorrow
• Mentally drafting an email to school, work, or a clinic
You put a show on.
You scroll.
You “relax.”
You get up again feeling… not rested at all.
Then you decide:
“I’m just bad at resting. I don’t know how to relax.”
No.
You are not bad at rest.
You are never actually off duty.
This article is about:
• Why so many women feel incapable of rest
• How the invisible mental load keeps you on call 24/7
• Why “doing nothing” doesn’t automatically equal recovery
• How to build real rest into a life that still has kids, work, clinics, hormones and bills
• How Sistapedia fits into this picture of women’s health, mental load and burnout
The Problem Isn’t That You Can’t Rest — It’s That You’re On Call All the Time
When you look at your day on paper, it might show:
• Work hours
• Family time
• Maybe a “break” or “self-care” block
In reality, behind all of that is a constant, invisible layer:
• Tracking who needs what and when
• Remembering appointments, birthdays, meds, sports, forms
• Pre-empting meltdowns, clashes, gaps, emergencies
• Strategising food, money, school, work, health, relationships
This invisible layer is often called the mental load or cognitive labour. It doesn’t switch off just because your body sits down.
So when you say “I’m resting,” what’s usually happening is:
• Your body is less active
• Your brain is still running a full system scan in the background
No wonder you stand back up feeling exactly the same.
Why Women in Particular Feel “Bad at Rest”
If you’re a woman (especially in your reproductive years and beyond), you’ve likely been trained to:
• Be useful
• Be available
• Be responsible for emotional and practical logistics
Messages sound like:
• “Mums don’t get days off.”
• “If you want something done properly, do it yourself.”
• “Women just multitask better.”
• “She’s the glue that holds everything together.”
Translation:
Your worth is tied to what you produce, fix, remember and hold for everyone else.
So when you attempt rest, three things collide:
1. Guilt:
• “I should be using this time better.”
• “The kids/partner/parents need me.”
• “Other people don’t have the luxury to rest.”
2. Anxiety:
• “What if I drop a ball?”
• “What if I forget something important?”
• “What if everything falls apart if I’m not watching?”
3. Practice:
• Your nervous system hasn’t had regular, safe experiences of being truly off duty.
• Of course it doesn’t know how to relax on command.
This isn’t a personal moral failure. It’s conditioning plus load.
Why Scrolling, TV and “Collapsing” Don’t Feel Like Real Rest
You finally get a moment without anyone needing you.
You collapse on the couch.
What do you reach for?
• Phone
• Remote
• Laptop
These things are not bad. But on their own, they usually give you escape, not rest.
Difference:
• Escape numbs you from how you feel for a short time.
• Rest helps your body and mind recover so you can function better afterwards.
If you finish a “rest” block feeling:
• Like your brain is still buzzing
• More wired or flat than before
• Guilty and behind on everything
…you probably escaped (understandable) but didn’t actually rest.
The Nervous System Side: You’re Stuck in “Always On” Mode
When you’re constantly scanning for:
• What’s next?
• Who needs me?
• What might go wrong?
…your nervous system spends most of its time in sympathetic activation — the “on guard” mode.
Signs:
• Difficulty falling asleep or staying asleep
• Waking up unrefreshed
• Feeling “tired but wired”
• Snapping quickly, then feeling guilty
• Getting sick often or carrying chronic pain/fatigue
To rest, your body needs at least some time in parasympathetic mode — the “safe enough to downshift” state.
You can’t logic yourself into that state. You have to create conditions that are:
• Safe enough
• Boundaried enough
• Supported enough
…for your system to stop acting like something bad might happen if you stop.
Step 1: Name the Fact — You’re Never Off Duty
Before you try any new routine or practice, be honest with yourself:
• How many hours in a day are you genuinely off call?
• No kids calling you
• No one expecting a reply
• No monitoring of other people’s needs
• No work notifications
For many women, the honest answer is:
“Almost zero.”
So instead of:
• “Why can’t I rest?”
A more accurate question is:
• “Why do I expect my body to know how to rest when it’s literally never off duty?”
This isn’t semantics. It’s clarity.
Once you name the problem correctly, you can design a realistic solution.
Step 2: Define What “Rest” Actually Means for You
Rest is not one-size-fits-all. You need a menu that suits:
• Your life stage (fertility, IVF, pregnancy, newborn, toddlers, teens, perimenopause, menopause)
• Your health (endo, PCOS, chronic pain, mental health, etc.)
• Your brain (ADHD/autism tendencies, anxiety, trauma history)
Think in four categories:
1. Physical Rest
• Sleep, naps, lying down, gentle stretching
• Doing nothing with your body on purpose
2. Mental Rest
• Time where you are not solving problems or planning
• Simple, absorbing activities with low stakes (e.g. simple crafts, light reading, audio stories)
3. Emotional Rest
• Time where no one is asking you to hold their feelings
• Spaces where you can be honest without caretaking
4. Sensory Rest
• Reduced noise, light, notifications, touch
• Even 5–10 minutes in a quiet room or outside without stimulation
Your “rest menu” might include:
• 20 minutes lying down with eyes closed and phone in another room
• Walking alone with a podcast you actually enjoy (not productivity content)
• Sitting outside with a drink, no devices, no talking
• A bath/shower with the door actually locked
• Short guided breathing or body scans
What matters is not how it looks from the outside. What matters is:
Does this bring my system down a notch?
Step 3: Build Micro-Rest Into a Life That Won’t Stop
You’re probably not getting a month-long wellness retreat. Fine.
Look for micro-rest blocks:
• 3 minutes in the car before you go inside
• 5 minutes sitting or lying down after you put a baby down
• 10 minutes between meetings with your phone on Do Not Disturb
In those micro-blocks, choose one thing:
• 10 slow breaths
• A quick stretch routine
• Lying flat and letting your body feel heavy
• Looking out a window and letting your eyes rest on something far away
This is not performative mindfulness. This is nervous system maintenance.
Step 4: Change the Rule From “Rest Last” to “Rest Is a Task”
Right now, rest is probably treated as:
• Optional
• A reward if everything else is done
• The first thing to go when the day gets complicated
Flip it:
• Put rest in your calendar as an actual block
• Treat it the way you treat a non-movable appointment for your child or a clinic
You won’t always hit it perfectly. But if it’s not even on the page, it will never happen.
Small script shift:
• From: “If I get time, I’ll rest.”
• To: “I have a rest block at X time. If something genuinely urgent displaces it, I move it, I don’t delete it.”
Step 5: Reduce “Background Tabs” Where You Can
You don’t just need more rest. You also need less load where possible.
Mini-audit:
• Which tasks are you doing purely because “I’ve always done them”?
• What could be:
• Automated? (subscriptions, reminders, direct debits)
• Delegated? (partner, kids, outsourced)
• Dropped? (unnecessary obligations, optional extras)
Examples:
• Use one shared family shopping list instead of tracking everyone’s preferences in your head.
• Create 3–5 “standard meals” in heavy weeks, and stop feeling bad about repetition.
• Unsubscribe from newsletters and WhatsApp groups you never read but feel guilty about.
Every background tab you close is future rest you’re buying.
Step 6: Guilt Management — You Can’t Rest and Self-Beat at the Same Time
Rest plus guilt is not rest.
You will feel guilty at first. Expect it.
Instead of arguing with the guilt, try:
• “Of course I feel guilty — I’ve been trained to. I’m still allowed to rest.”
• “Someone being slightly inconvenienced so I don’t burn out is an acceptable trade.”
• “Me being less exhausted is good for everyone in this house.”
Remind yourself:
Children don’t need a parent who never sits down.
They need a parent who is not fried to a crisp all the time.
How Sistapedia Fits In: Rest Is a Reproductive Health Issue
This isn’t just a lifestyle problem. It’s a health problem.
Chronic lack of rest and constant mental load intersect with:
• Fertility and TTC
• IVF and medical treatment
• Endometriosis, PCOS and chronic pain
• Pregnancy, postpartum, breastfeeding
• Perimenopause and menopause
• Mental health (anxiety, depression, burnout)
Sistapedia® is being built specifically at this intersection:
A global, AI-verified marketplace and social platform for women’s reproductive health — not just organs and hormones, but the reality of how you live inside them.
For Sistas (You)
On Sistapedia, you can:
• Talk honestly about the fact that you are never off duty
• Share what “rest” looks like when you have kids, chronic conditions, fertility treatment, or caring responsibilities
• Read AI-verified content from Crown Verified experts on stress, hormones, sleep, mental load and burnout
💖 When you share your lived experience and help other women feel less defective for struggling with rest, you can apply for your free Pink Tick — our verification for Sistas building an honest sisterhood around reproductive health.
For Experts & Practitioners
If you’re a:
• GP, psychologist, psychiatrist or counsellor
• Endocrinologist, gynaecologist, fertility specialist or menopause clinician
• Pain specialist, physio, dietitian or coach working with women’s health
…Sistapedia is where you can:
• Create a professional profile
• Share evidence-based guidance on rest, nervous system health and reproductive health
• Apply to become Crown Verified — our verification for qualified experts, clinics and services in women’s health.
👑 Crown Verification tells Sistas that you understand rest as a clinical issue, not just vague “self-care.”
Final Thoughts: You Don’t Need to Be Better at Rest — You Need Permission to Be Off Duty
If you’ve been thinking:
• “I’m just terrible at relaxing.”
• “Even when I stop, I don’t feel rested.”
• “What’s wrong with me that I can’t just switch off?”
…there’s a high chance there is nothing wrong with you.
You are:
• Carrying a mental load that never stops
• Running a nervous system that’s constantly on guard
• Living in a culture that praises your output and quietly punishes your rest
You don’t need to become a different person. You need:
• Some of your load externalised, shared or dropped
• Safe micro-moments where you are genuinely off call
• A story about rest that doesn’t frame you as lazy for needing it
✨ Join Sistapedia, your global sisterhood, and step into a space where being “never off duty” is treated as data — not a personality flaw.
Parenting When You’re the Only One With a Diagnosis: ADHD, Autism, Chronic Illness and the Motherhood Mental Load

ADHD mum mental load
You’re running a whole family on a brain or body with limits.
Maybe you’ve been diagnosed with:
• ADHD
• Autism
• A chronic illness (pain, fatigue, autoimmune, migraines, etc.)
Or you strongly suspect you’re neurodivergent or chronically ill — even if no one’s put it in writing yet.
You’re still:
• Booking appointments
• Packing lunches
• Tracking school emails
• Remembering sports uniforms, birthday parties, due dates, medical forms
You’re the system admin of the household… with a nervous system that often feels like it’s running on 3% battery.
And there’s this extra twist:
You’re the only one with a diagnosis.
Your kids, partner, extended family and school can all default to:
• “You’re the adult, you should cope.”
• “You just need to be more organised.”
• “You’re overthinking / overreacting / too sensitive.”
This article is for the parent (usually the mum) who’s:
• Carrying the mental load
• Managing ADHD, autism or chronic illness
• Being treated like both the problem and the solution
We’ll cover:
• Why the mental load hits harder when you’re the diagnosed one
• How ADHD/autism/chronic illness change the day-to-day realities of parenting
• The guilt and shame loops that keep you over-functioning until you crash
• Practical strategies to redesign your systems, not just “try harder”
• How to talk to your family, school and yourself about your limits
The Hidden Rule: “You’re the Diagnosed One, So You Have to Work Around Everyone Else”
If you’re the only person in your household with a label, the unspoken rule often becomes:
• Everyone else is “default normal”
• You’re the “difficult one”
• The system doesn’t change — you are expected to change
That can look like:
• You masking ADHD or autistic traits so no one else has to adjust
• You pushing through chronic pain or fatigue so routines stay “normal”
• You absorbing all the admin and emotional labour because “you’re home more” or “you care more”
When you try to advocate for your needs, you’re told:
• “You’re making it about you.”
• “The kids need stability, you can’t be inconsistent.”
• “Maybe this is just parenting, everyone is tired.”
So you end up:
• Gaslighting yourself
• Overriding your own body and brain
• Running on adrenaline and hyper-focus until you crash
The problem isn’t your diagnosis. The problem is a system that refuses to acknowledge it.
How ADHD Changes the Mum Mental Load
ADHD isn’t just “distracted” or “hyper.” It affects:
• Working memory (keeping multiple steps in mind)
• Task initiation (starting things)
• Task switching (changing tasks without dropping balls)
• Time perception (“I have no idea how long anything takes”)
Now drop that into:
• School emails
• Sports schedules
• Medical appointments
• Lunches, laundry, bills, birthday.
You’re expected to run what is essentially a project management role with an executive-function system that’s wired differently.
That can mean:
• You know what needs to be done but feel physically blocked from starting
• You start five tasks at once and finish none
• You miss small admin things and then feel like a failure
• You get overwhelmed and doom-scroll because your brain can’t pick a starting point
It’s not laziness. It’s a brain architecture mismatch between what modern motherhood demands and the cognitive style you have.
How Autism Changes the Mum Mental Load
Autism can bring:
• Sensory sensitivity (noise, touch, visual clutter)
• Social fatigue from school gates, birthday parties, playdate politics
• Need for structure + predictability
• Intense focus on some tasks and total shutdown with others
Parenting demands:
• Constant sensory exposure (noise, mess, movement)
• Emotion coaching for kids when you might be overloaded yourself
• Unwritten social rules in parent groups, schools, sports
• Flexibility around last-minute changes and chaos
You might:
• Hold it together all day, then meltdown once kids are in bed
• Avoid certain events because recovery time is too high
• Feel like a “bad mum” because noisy play or messy activities are physically painful
• Mask hard at school events and pay for it with days of exhaustion
Again: not a character flaw. It’s a nervous system doing too much processing 24/7.
How Chronic Illness Changes the Mum Mental Load
Chronic illness can bring:
• Pain
• Fatigue
• Brain fog
• Unpredictable “crash” days
But the world still expects you to:
• Show up consistently
• Be emotionally available
• Keep the house running
• Plan, remember, manage, track everything
That leads to:
• Saying “yes” to everything so your kids don’t “miss out”
• Paying for it with flare-ups that they also witness
• Guilt if you have to cancel or lie down instead of playing or helping
You might feel like your body is the limiting factor in your family’s life, and that’s a heavy weight to carry.
The Guilt & Shame Loop: “If I Just Tried Harder…”
ADHD, autism and chronic illness all come with one predictable side-effect: self-blame.
Internal monologue usually sounds like:
• “Other mums can do this; what’s wrong with me?”
• “My kids deserve someone more patient / organised / healthy.”
• “The diagnosis explains things, but I should be coping better.”
So you:
1. Over-function to prove you’re not “using it as an excuse”
2. Crash (symptom flare, meltdown, shutdown, burnout)
3. Feel ashamed
4. Vow to “do better” next time
5. Repeat
Your kids don’t need a mum who pretends to be superhuman and then disappears into collapse. They need:
• Realistic capacity
• Honest communication
• Systems that don’t rely on you being at 200% all the time
System Redesign: Stop Being the Only Grown-Up in the House
You cannot rely on willpower and chaos management forever. You need systems that match your brain/body.
Externalise the Family Brain
Get things out of your head and into shared visibility:
• A big family calendar (paper on the wall or shared digital)
• Colour-code each person
• Put everything on it: work shifts, appointments, homework deadlines, sports, social events
Make it a rule:
“If it’s not on the calendar, it doesn’t exist.”
Everyone contributes. You are not the only updater.
Reduce Decision Load with Default Routines
Decisions burn energy — especially with ADHD/autism/chronic illness.
Pick defaults for:
• Meals (e.g. themed nights: pasta Monday, tacos Tuesday, etc.)
• Laundry (specific days / times)
• School prep (always done right after dinner, not “some time tonight”)
You’re not failing by simplifying. You’re designing for sustainability.
Delegate Like You’re the CEO, Not the Housemaid
If kids are old enough to:
• Use a tablet
• Navigate games
• Operate a TV remote
…they’re old enough for age-appropriate jobs.
Examples:
• Primary school kids:
• Pack their own bag using a checklist
• Put dirty clothes in hampers
• Put lunchboxes on the bench after school
• Older kids:
• One or two fixed weekly chores (bins, dishwasher, pet care)
• Help with simple meals
• Own their sports gear organisation
Your diagnosis is not a reason to do more for everyone. It’s a reason to make household roles more equitable.
Talking to Your Kids About Your Diagnosis (Without Burdening Them)
You don’t have to share everything, but age-appropriate honesty can:
• Reduce confusion (“Why is Mum tired/cranky/forgetful?”)
• Reduce self-blame (“Did I cause this?”)
• Model self-acceptance and boundaries
Simple scripts:
For ADHD:
“My brain is a bit like having 20 tabs open at once. It means I can be very creative and think of lots of ideas, but it also means I sometimes forget things or get overwhelmed. That’s why we use lists and calendars — so my brain doesn’t have to hold everything alone.”
For Autism:
“My brain notices sounds, lights and feelings really strongly. That can be amazing for details and creativity, but it can also make noisy places hard. If I need quiet time or headphones, that’s me taking care of my brain.”
For chronic illness:
“My body has a health condition that means I get tired / sore faster than other people. It’s not your fault. When I lie down or say no to an activity, that’s me looking after my body so I can still be your mum for a long time.”
You’re not asking them to parent you. You’re teaching them reality and boundaries.
When to Pull in External Support (And Why That’s Not Failure)
Signs you need more support:
• You’re melting down regularly in front of your kids from overload
• Basic tasks (meals, washing, school admin) feel unmanageable most weeks
• You’re snapping, withdrawing or going numb frequently
• Your health is clearly getting worse under the load
Options (depending on finances and location):
• ADHD / autism-informed therapist or coach
• Occupational therapist for practical strategies
• Pain/fatigue clinic or specialist for chronic illness
• NDIS or disability supports where applicable (if you’re in a system that offers this)
• Cleaning help or meal services, even short-term, if budget allows
Outsourcing is not “cheating motherhood.” It’s building a scaffold around a nervous system that’s already doing too much.
How Sistapedia Fits In: Your Diagnosis + Motherhood Are Not Niche
Parenting with ADHD, autism or chronic illness is not a side story — it’s central to how real families operate.
Sistapedia® is being built for exactly this kind of reality:
• ADHD, autism and chronic illness in women
• Fertility, pregnancy, postpartum and parenting
• Hormone health, periods, perimenopause and menopause
• Mental load, medical gaslighting and system-level gaps
For Sistas (You)
On Sistapedia, you can:
• Share what it’s like to run a household with a neurodivergent or chronically ill brain/body
• Give and receive practical hacks that actually work with ADHD/autistic wiring and low-energy days
• Access AI-verified content and Q&As around women’s health, parenting and diagnosis that aren’t written for “generic” mums
💖 When you share your lived experience and help other women feel less defective, you can apply for your free Pink Tick — our verification for Sistas who are turning their story into community impact.
For Experts & Practitioners
If you’re a:
• Psychologist, psychiatrist, paediatrician or GP
• ADHD / autism coach or OT
• Chronic pain / fatigue specialist
• Family therapist, social worker or parent educato
…Sistapedia is where you can:
• Create a professional profile
• Share evidence-based strategies for parenting when the parent has a diagnosis
• Apply to become Crown Verified — our verification for qualified experts, clinics and services in women’s health and parenting.
👑 Crown Verification signals that you understand neurodivergent and chronically ill motherhood as real, not “excuses.”
Final Thoughts: You Are Not a Broken Version of a “Real Mum”
If you’re parenting with ADHD, autism or chronic illness and you’re the only one with a diagnosis, it can feel like you’re constantly failing some invisible standard.
You’re not.
You’re:
• Running a household on hard mode
• Doing unpaid labour as project manager, emotional regulator and logistics officer
• Doing it all with a brain and/or body that the system never planned for
You deserve:
• Systems that match you
• Kids who see you as human, not superhuman
• A story that doesn’t cast you as the problem
✨ Join Sistapedia, join the sisterhood, and step into a space where your diagnosis and your motherhood are both taken seriously.
Perimenopause and Work Performance Anxiety: Handling Brain Fog, Memory Slips and Meetings in Your 40s

Perimenopause Brain Fog at Work
You’re in your 40s, sitting in a meeting you could have run in your sleep ten years ago.
You used to be:
• The one who remembered every detail
• The fastest problem-solver in the room
• The person others leaned on for clarity
Now you’re:
• Losing words mid-sentence
• Forgetting what you were about to say
• Re-reading the same email three times
• Dropping small balls you never used to drop
On the outside, you’re still functioning.
On the inside, you’re thinking:
“Am I burning out? Am I getting early dementia? Has everyone noticed I’m not as sharp?”
For many women in their late 30s and 40s, this is perimenopause colliding with work — and the anxiety it creates can be just as damaging as the symptoms.
This article covers:
• What perimenopause actually is (beyond “one day you stop bleeding”)
• How hormonal shifts can affect focus, memory, language and confidence
• Why performance anxiety spikes at exactly the stage you’re supposed to be “at your peak”
• Practical strategies you can use in meetings, deep-focus work and busy weeks
• How to talk (or not talk) about it at work without torching your reputation
This is general information, not individual medical advice. Always talk to a qualified clinician about your own symptoms and treatment options.
Perimenopause 101: You’re Not Imagining the Shift
Perimenopause is the transition phase leading up to menopause (the point when you’ve gone 12 months without a period).
It can start:
• As early as your mid-30s for some women
• More commonly in your 40s
And can last anywhere from a couple of years to close to a decade.
Key point:
Hormones don’t slide down in a straight, graceful line. They fluctuate — sometimes wildly.
Estrogen and progesterone levels can surge and crash, which affects:
• Sleep
• Mood
• Temperature regulation (hello, hot flushes)
• Pain sensitivity
• And yes, how your brain functions day-to-day
So if you’re feeling different in your 40s — not just in your body, but in your mental sharpness — that’s not you being dramatic. That’s physiology.
What Perimenopause Brain Changes Can Look Like at Work
Women often describe:
• Word-finding issues:
• “I know exactly what I mean but can’t find the word.”
• Short-term memory slips:
• Walking into a room and forgetting why
• Losing track of what you were saying mid-sentence
• Concentration problems:
• Reading the same paragraph repeatedly
• Struggling to follow long, dense conversations or documents
• Mental fatigue:
• Feeling “done” much earlier in the day than before
• Sleep-related fog:
• Waking at 2–4 am and then pushing through a full workday
None of this means you’ve lost your intelligence, skills or experience. It means:
• Your brain is working under different hormonal conditions
• Your sleep quality may be compromised
• Your nervous system is carrying more load (career, caregiving, aging parents, teen kids, health worries)
The problem is not that you’re suddenly incapable.
The problem is that the environment around you rarely adjusts.
Why Performance Anxiety Blows Up in Your 40s
Perimenopause hits at the exact life stage where many women are:
• In or approaching senior roles
• Carrying major financial responsibilities
• Managing kids, teenagers, partners, and aging parents
• Expected to be “rock solid” and “a safe pair of hands”
So when brain fog, memory slips or emotional swings appear, it can trigger:
• Fear of being seen as past your peak
• Fear of being replaced by younger colleagues
• Fear of confirming stereotypes about women being “too emotional” or “unstable”
This performance anxiety can then amplify itself:
• Worrying about messing up → more adrenaline → worse sleep → more fog → more mistakes → more worry
You end up in a loop where you question your identity as the competent, capable one.
Important reality check:
Experiencing perimenopause symptoms does not erase the 15–25 years of expertise you’ve built. It adds friction — it doesn’t erase value.
Step 1: Track What’s Actually Happening (Not Just How It Feels)
When anxiety is high, it’s easy to catastrophise:
• “I’m messing everything up.”
• “I’m not good at my job anymore.”
Before you rewrite your whole story, get some data:
• For 2–4 weeks, jot down:
• When you feel foggy (time of day, cycle day if you still track)
• Sleep quality (hours, night wakings)
• Specific situations where you blank (e.g. large meetings vs 1:1, reading vs speaking)
• Caffeine, alcohol and stress spikes
Patterns often emerge:
• Fog is worst after multiple nights of poor sleep
• Word-finding issues cluster at certain cycle phases
• Large, fast-moving meetings are harder than deep-focus solo work
This isn’t to blame or “biohack” your way out of perimenopause — it’s so you can be strategic, not self-loathing.
Step 2: Get a Proper Medical Check, Not Just “You’re Just Getting Older”
Do not accept a shrug if:
• Symptoms are affecting your work and quality of life
• You’re dealing with brain fog, sleep disruption, mood swings, heavy or erratic bleeding, hot flushes or joint pain
A good clinician will:
• Take a detailed history (cycles, symptoms, mood, sleep, family history)
• Consider blood tests (not as a one-off “yes/no” for perimenopause, but as part of the picture)
• Check for other contributors:
• Thyroid issues
• Iron deficiency or anemia
• Vitamin B12 or D deficiency
• Sleep disorders, depression, anxiety
Then you can discuss treatment options, which may include:
• Hormone therapy (if appropriate and safe for you)
• Non-hormonal medications for specific symptoms (e.g. hot flushes, mood, sleep)
• Targeted lifestyle changes that are realistic for your life stage
You’re not “bothering” anyone by asking for help. Your brain, job and relationships are on the line.
Step 3: Tactical Adjustments for Workdays (Brain Fog Edition)
You can’t reorder your hormones on demand, but you can adjust how you work.
1. Externalise Everything You Can
Stop relying on your brain as a storage device. Use:
• Calendar reminders (with more detail than you think you need)
• Task lists broken into micro-steps
• Meeting prep notes with key points written out, not just in your head
Before important meetings:
• Write down the 3 main points you want to make
• Keep that in front of you so you can glance down when words disappear
This is not a downgrade. This is a professional using tools.
2. Protect Your Deep-Focus Windows
If you notice:
• You’re sharper in the morning → protect a 60–90 minute block most days for high-cognition work
• You fade after lunch → schedule admin, emails or lower-stakes tasks then
Where you can, avoid:
• Booking back-to-back high-stakes meetings in your worst brain window
• Forcing concentration when you’re already obviously fried
You may not have perfect control, but even small shifts help.
3. Use Simple Grounding in the Moment
When you blank in a meeting, anxiety spikes. To interrupt the spiral:
• Pause, take a slow breath, and use a bridging phrase:
• “Let me just pull that back together for a second…”
• “I want to make sure I phrase this clearly — what I’m trying to say is…”
• Glance at your notes and keep going
Most people are far more focused on themselves than on your brief pause.
Step 4: Decide How (and Whether) to Talk About It at Work
You do not have to disclose perimenopause at work if you don’t want to. It’s private health information.
Options range from:
1. Say nothing medical, just describe impact:
• “I’m dealing with some health-related sleep issues at the moment. I’m still committed to my role, but I may need to rely more on written checklists and occasional schedule tweaks while I work through it with my doctor.”
2. Name “hormonal changes” without specifics:
• “I’m dealing with some hormonal changes that are affecting my sleep and concentration on some days. I’ve got medical support, but I may need a bit more flexibility with big meeting timing over the next few months.”
3. Explicitly name perimenopause (only if it feels safe):
• “I’m in perimenopause, and it’s affecting my sleep and focus on some days. I’m undergoing treatment, and most of the time I’m fine, but I wanted you to know why I’m making some changes to how I structure my work.”
Your decision should be based on:
• Your manager’s track record with health disclosures
• The culture of your organisation
• Your legal protections (or lack of) around age, gender and health discrimination
If your gut says “this will be weaponised against me,” focus on describing functional needs, not labels.
Step 5: Challenge the “Peak at 40, then Decline” Story
Perimenopause brain changes can make you feel like:
• “I’ve peaked, it’s all downhill.”
• “Younger colleagues are the future; I’m the past.”
Reality:
• Your 15–25 years of experience, context and pattern-recognition are huge assets.
• Many women restructure their careers in their 40s/50s, not because they’re failing, but because they’re done tolerating bad systems.
• Once symptoms are properly recognised and treated, many women report a significant improvement in cognitive function and energy.
It’s not that you’re suddenly “not good enough.” It’s that:
• The system expects you to be 25 forever
• There’s almost no built-in support for the physiological transitions half the workforce will experience
You’re allowed to be angry at that, not just afraid.
How Sistapedia Fits In: Your Brain Fog Is Data, Not Just “A Phase”
Perimenopause + work performance anxiety is exactly the kind of reality Sistapedia® is built around.
We’re creating the world’s first AI-verified marketplace and social platform focused solely on women’s reproductive health across the full lifecycle:
• Periods, contraception, PCOS and endometriosis
• Fertility, IVF, pregnancy and postpartum
• Perimenopause, menopause and long-term health
For Sistas (You)
On Sistapedia, you can:
• Share what perimenopause at work actually feels like — the forgotten words, the performance reviews, the quiet panic
• Read other women’s strategies for managing brain fog, sleep issues and meetings without self-destructing
• Access AI-verified content and Q&As that don’t treat perimenopause as an afterthought
💖 When you share your story and support others, you can apply for your free Pink Tick — our verification for Sistas whose lived experience is helping re-write the script on midlife, work and hormones.
For Clinicians, Coaches, Employers & Experts
If you’re a:
• GP, menopause specialist, endocrinologist or psychiatrist
• Workplace psychologist, leadership coach or HR leader
• Organisation designing menopause and midlife policies
…Sistapedia is where you can:
• Create a professional profile
• Share evidence-based strategies for supporting perimenopausal women in the workforce
• Apply to become Crown Verified — our verification for qualified experts, clinics, services and organisations in women’s reproductive health.
👑 Crown Verification signals that you understand perimenopause as a serious health and work issue — not just “a few hot flushes.”
Final Thoughts: You’re Not “Losing It” — You’re Moving Into a New Phase
If you’re blanking in meetings, misplacing words and feeling like a stranger to your own brain, you’re not broken and you’re not alone.
You’re a woman in a body that is:
• Changing hormonally
• Carrying heavy responsibilities
• Operating in systems that barely recognise any of it
You deserve:
• Proper assessment and treatment
• Adaptations that let you keep using your expertise
• A narrative that doesn’t end your story at 45
✨ Join Sistapedia, the global sisterhood, and step into a space where perimenopause and work aren’t separate conversations — they’re finally part of the same reality.
What a Fertility-Friendly Workplace Would Look Like (So You Notice When Yours Isn’t)

Fertility-Friendly Workplace
You’re trying to grow your family and your career at the same time.
On paper, that sounds empowering. In real life, it can feel like:
• 6:30 a.m. blood tests
• 8:30 a.m. stand-up meetings
• Midday ultrasounds hidden as “dentist” appointments
• Afternoons pretending you’re not exhausted, bloated or on the edge of tears
If your workplace isn’t explicitly fertility-friendly, IVF and egg freezing can become a secret second job:
• Juggling meds, scans and procedures around meeting calendars
• Carrying the emotional load of each cycle in silence
• Worrying that time off or reduced performance will hurt your reputation
This article walks through:
• What “fertility-friendly” workplaces actually look like (and why so few exist)
• How to plan IVF / egg freezing when your job isn’t built for it
• Whether, when and how to disclose to a manager or HR
• Scripts you can use if you do decide to tell someone
• Boundaries to protect your mental health and career while you’re in treatment
This is general guidance, not legal advice. Workplace rights vary by country and contract, so always check your local laws and your employer’s policies.
What a Fertility-Friendly Workplace Would Look Like (So You Notice When Yours Isn’t)
Before we talk survival strategies, it helps to name the gap.
A genuinely fertility-friendly workplace usually has:
• Flexible hours for early-morning bloods and ultrasounds
• No penalty (overt or subtle) for using sick leave or personal/carer leave for treatment
• Understanding from managers that IVF and egg freezing can involve sudden timetable changes
• Confidential HR processes for health-related leave
• No fertility shaming (“you’re so lucky, I wish I could take time off for that”)
• Sometimes even formal policies around fertility treatment, pregnancy loss and family forming (including solo parents and LGBTQIA+ families)
Most workplaces are… not there yet.
Instead, women report:
• Feeling judged for “too many appointments”
• Being expected to make up hours in the evenings
• Hearing comments like “we can’t keep covering for you”
• Fearing that being open about IVF will cost them promotions
You’re not oversensitive if your workplace doesn’t feel safe to be honest about treatment. You’re noticing a structural problem, not a personal weakness.
Step 1: Get Clear on Your Treatment Demands
It’s hard to navigate work if you don’t know roughly what’s coming.
Ask your fertility specialist or clinic:
“What does a typical cycle look like for someone in my situation?”
• How many appointments?
• What time of day are bloods/scans usually done?
• How much notice do I get?
“Which parts definitely need time off, and for how long?”
• Egg collection
• Embryo transfer
• Recovery time
“What side effects might affect my work capacity?”
• Fatigue, bloating, mood swings, headaches, nausea
Get a realistic view of:
• How many early starts
• How many mid-day absences
• How many full or half days off for procedures
You’re not being “difficult” by asking. You’re planning.
Step 2: Decide If You’ll Disclose — and to Whom
There’s no one right answer here. Disclosure is a strategic decision, not a moral test.
Broad options:
1. Tell no one
• Pros: privacy, no awkward questions, no stigma if workplace is unsupportive
• Cons: you carry everything alone, harder to explain unpredictable absence or performance dips
2. Tell one trusted person (usually your direct manager or HR)
• Pros: can negotiate flexible arrangements, less need to lie or over-explain
• Cons: requires vulnerability; depends heavily on that person’s attitude
3. Tell a small, carefully chosen circle
• e.g. manager + HR, or manager + one key colleague
• Pros: spreads understanding; gives you more practical backup for meetings and deadlines
• Cons: more people in the loop; privacy risk if your workplace culture is loose about gossip
Questions to ask yourself:
What’s my manager’s track record with health/personal issues?
Does my company have any existing policies on fertility, IVF, pregnancy loss or carers’ leave?
Would knowing give my manager more capacity to protect me, or just more power over me?
If your gut says, “This person will use this against me,” protect yourself and stay minimal.
Step 3: If You Do Decide to Tell Your Manager — Use a Clean Script
You don’t have to provide medical essays.
Here are a few options you can adapt.
Short, Minimal Disclosure
“I wanted to let you know I’m undergoing a time-sensitive medical treatment over the next few months. It will involve early-morning and occasional short-notice appointments. I’m still committed to my role and happy to plan proactively so work continues smoothly, but I may need some flexibility around start times and occasional short absences.”
If they press for detail and you’re not ready:
“It’s a reproductive health issue and I’d prefer to keep the specifics private, but I wanted you to understand why there are extra appointments.”
Slightly More Specific (Naming Fertility Treatment)
“I’m going through fertility treatment (IVF/egg freezing) over the next few months. That means early scans and blood tests that are often scheduled with little notice, plus a couple of procedure days where I’ll need time off. I’d like to work with you to plan around key dates and make sure our priorities are covered.”
If they respond well, you can build from there. If they don’t, you’ve still kept details relatively contained.
Step 4: Plan Around “Known Unknowns”
Treatment has unpredictable parts, but some patterns are predictable enough to plan around.
1. Map Critical Work Periods vs Likely Treatment Windows
• Busy season, product launches, exams, board meetings, big pitches
• Approximate stimulation and procedure windows for your cycles
See where they overlap and ask:
“Can I choose a cycle start date that avoids the worst clash?”
“Can we schedule the largest deliverables outside my most intense treatment weeks?”
Sometimes the answer will be no. But sometimes small shifts make a big difference.
2. Build Backup Plans for “What If” Days
For key responsibilities, identify:
• Who can step in if you’re unexpectedly out for a day?
• What absolutely must not fail (client meeting, exam, deadline)?
• What can be delayed, delegated or dropped?
Write this down and share it with your manager if you’ve disclosed. Don’t assume they’ll figure it out on the day.
Step 5: Protect Your Mental Health While You’re Still at Your Desk
IVF and egg freezing are not just logistics. They’re loaded with hope, fear, grief and hormones.
Practical boundaries that help:
1. Decide Where You’ll Read Results
If your clinic delivers results by phone, portal or email:
• Choose whether you want to see them at your desk, in a bathroom, at home, or parked in your car.
• If results are likely mid-workday, consider stepping out for 10–15 minutes when you know they’re coming.
You’re allowed to protect yourself from falling apart in open-plan.
2. Pre-Plan Your Exit Strategy for Bad-News Days
Ask yourself:
“If this cycle fails, what’s the bare minimum I have to do today at work?”
“Can I give myself permission to take sick leave or log off early?”
You do not owe your employer your best performance on the day your IVF cycle collapses or you get a devastating call.
3. Limit Fertility Content During Work Hours
Constantly scrolling fertility forums and negative test videos between tasks won’t help your nervous system.
You can:
• Mute or hide certain hashtags during work hours
• Set a rule like “I only look at fertility stuff at lunch / after work”
• Use app blockers if you need hard boundaries
Not because you don’t care — but because you do, and you need mental bandwidth to function.
Step 6: Handling Comments, Curiosity and Boundary Crossers
If you’ve disclosed, some colleagues will be kind, some neutral, and some… clumsy.
You’re allowed to set boundaries.
Polite but Firm Responses
If someone asks for details you don’t want to share:
“It’s a bit personal for me to go into, but I appreciate your support.”
If someone makes a minimising joke (“Must be nice taking all that time off”)
“It’s actually pretty intense medical treatment, not time off. I’m doing my best to keep work on track as well.”
If people keep asking, “Any news?”
“I’ll share if and when I’m ready. For now I’d rather keep it off the office radar.”
You don’t owe anyone ongoing updates just because you disclosed once.
Step 7: Watch for Burnout and Know Your Red Lines
Signs you’re burning out:
• Crying before or after work most days
• Dreading both work and appointments
• Making frequent mistakes because you’re emotionally and physically depleted
• Feeling resentful and trapped, like there’s no oxygen in either part of your life
If this is you, something has to give — temporarily or permanently.
Possible levers (depending on your situation):
• Short-term leave (sick, personal, unpaid, or fertility-specific if your employer offers it)
• Reducing hours for a set period
• Requesting a temporary role adjustment
• In some cases, seriously assessing whether this workplace is compatible with your long-term health and family goals
None of these options are easy. But your body is not a machine that can indefinitely absorb two full-time jobs (work + fertility treatment) without consequences.
How Sistapedia Fits In: Work + Fertility Is a System Problem, Not Just a You Problem
Trying to do IVF or egg freezing in a non-fertility-friendly workplace is exactly the kind of “quiet crisis” Sistapedia® exists to surface.
We’re building the world’s first AI-verified marketplace and social platform focused entirely on women’s reproductive health and reality:
• Fertility, IVF, egg freezing and donor conception
• Pregnancy, birth and postpartum
• Endometriosis, PCOS, chronic pelvic pain and heavy periods
• Perimenopause, menopause and beyond
For Sistas (You)
On Sistatedia, you can:
• Share what it’s really like to do IVF/egg freezing alongside a demanding job
• Read strategies from other women who’ve negotiated flexible work, leave and disclosure
• Access AI-verified content on fertility, workplace health and rights (linked to Crown Verified experts where appropriate)
💖 When you share your story and support other women, you can apply for your free Pink Tick — our verification for Sistas whose lived experience is helping change how workplaces and clinics treat women.
For Employers, HR, Fertility Clinics and Professionals
If you’re a:
• Fertility specialist or clinic manager
• HR lead, people & culture director or workplace wellbeing lead
• Employment lawyer, psychologist, coach or occupational health clinician
…Sistapedia is where you can:
• Create a professional profile
• Share practical guidelines for truly fertility-friendly workplaces
• Apply to become Crown Verified — our verification for qualified experts, services and organisations working in women’s reproductive health and work-life integration.
👑 Crown Verification signals to Sistas that you are committed to evidence-based, ethical support — not box-ticking policies.
Final Thoughts: You’re Not “Too Much” for Needing Both Work and Fertility Support
If you’re holding spreadsheets in one hand and hormone injections in the other, you are not overreacting to feel exhausted.
You’re trying to build a future family in a system that still assumes workers don’t bleed, inject, miscarry or stim.
You deserve:
• A plan
• Some flexibility
• Real support, not just “good luck”
✨ Join Sistapedia, join the global sisterhood, and step into a space where your IVF calendar and your work calendar can finally be talked about in the same conversation — without shame.
AI Period & Symptom Trackers in 2025: How Accurate Are They for PCOS, Endometriosis and Irregular Cycles?

AI period tracker accuracy
You open your app and it confidently tells you:
• Your period will start in 3 days
• You’ll ovulate on day 14
• Your “fertile window” is green this week
Except:
• Your period turns up a week early.
• You’re spotting on “safe” days.
• Your cycle length jumps from 26 to 45 days with no warning.
If you live with PCOS, endometriosis, hypothalamic issues or generally chaotic cycles, you’ve probably already realised this:
Most period apps were built for textbook cycles — not for women like you.
Now they’re adding AI on top and promising “smarter” predictions and “personalised” insights.
This article breaks down:
• What AI period & symptom trackers actually do
• Why they can be wildly wrong for irregular cycles
• The difference between “pattern-spotting” and “medical assessment”
• How to use these apps as tools, not oracles
• Red flags that mean you shouldn’t rely on your app for contraception or fertility decisions
What AI Period & Symptom Trackers Actually Do (Under the Hype)
The marketing language sounds impressive:
• “AI-powered predictions”
• “Smart fertile window detection”
• “Deep learning for your hormones”
Underneath, most apps are still doing three basic things:
1. Collecting data you enter
• Period start/end dates
• Symptoms: pain, mood, discharge, spotting, headaches, libido
• Sometimes temperature, LH tests, cervical mucus, medication use
2. Spotting patterns in that data
• Average cycle length
• Typical luteal phase length (if they track ovulation surrogates)
• Recurring symptoms around specific days
3. Predicting future events based on past patterns
• “You usually bleed every 29 days → we’ll assume the next one is similar.”
• “You usually log headaches 2 days before bleeding → we’ll flag that as a pattern.”
Adding “AI” (machine learning, sometimes large language models) mainly improves:
• How well they fit curves to your past data
• How they cluster symptoms and surface patterns
• How nicely they explain things back to you in natural language
It does not suddenly give them:
• Access to your actual hormone levels
• The ability to detect endometriosis or PCOS from tracking alone
• Perfect ovulation timing in irregular cycles
They are still prediction engines, not diagnostic devices.
Why AI Trackers Struggle With PCOS, Endometriosis and Irregular Cycles
1. They Assume Some Level of Regularity
Even the more advanced apps are built on the assumption that your body has some repeating pattern.
With PCOS or hypothalamic dysfunction, you might have:
• 28-day cycle
• 35-day cycle
• 60-day cycle
• No period for months
• Then a random bleed out of nowhere
There may be no stable underlying pattern for the app to lock onto. It’s like trying to learn a song where the tempo changes every bar.
Result: the app “learns” an average that doesn’t exist in real life — and your predictions swing between false reassurance and false alarm.
2. Ovulation Predictions Are Often Weak Guesses
Many apps do one of two things:
• Predict ovulation as “cycle length minus 14 days” (the classic day-14 assumption dressed up in nicer UI), or
• Move ovulation around based on when you say your period arrived, assuming a normal luteal phase.
But:
• Luteal phase length isn’t identical in everyone.
• In PCOS or disrupted cycles, ovulation may happen late or not at all.
• Bleeding doesn’t always mean you’ve ovulated (e.g. anovulatory bleeding).
Apps that don’t incorporate objective ovulation markers (e.g. LH tests, BBT curves) are essentially giving calendar-based guesses with nicer fonts.
3. Pain and Symptom Clusters Can Be Misleading
If you log:
• Pain
• Fatigue
• Bowel symptoms
• Spotting
…your app might cluster this as “PMS” or “likely period starting soon.”
With endometriosis, adenomyosis or IBS overlap, those symptoms can show up throughout the cycle, not just pre-period.
So the app may:
• Over-call period starts
• Underestimate serious, non-cycle-related pain
• Reassure you when you actually need medical review
AI is only as good as the patterns in its training data. If that data under-represents complex conditions, the outputs will too.
What AI Trackers Are Good For — Even With Irregular Cycles
They’re not useless. They’re just limited.
Here’s where they can genuinely help you:
1. Symptom Diaries Without Paper Chaos
If you live with:
• PCOS
• Endometriosis
• PMDD
• Chronic pelvic pain
…long-term patterns matter. Digital tracking can help you:
• Remember when specific symptoms happened
• Show a doctor concrete data instead of trying to recall from memory
• Link symptoms to possible triggers (sleep deprivation, food, stress, exercise, meds)
The AI layer can sometimes surface patterns you hadn’t noticed, e.g.:
• “You usually report migraines 1–2 days before bleeding.”
• “Your worst pain days cluster around mid-cycle and pre-period.”
That’s useful in consults.
2. Planning Around Probabilities, Not Certainties
Even if your cycle isn’t consistent, trend-level info can help with:
• Roughly predicting when you might be premenstrual (for planning big events, work deadlines, travel)
• Recognising recurring “bad weeks” and building in buffer
• Identifying months where things are more extreme so you can ask, “What changed?”
Think of it as a weather forecast, not a train timetable.
3. Cycle-Literacy and Body Awareness
For some Sistas, just:
• Seeing their cycle laid out visually
• Learning the phases (follicular, ovulatory, luteal)
• Linking mood/energy changes to hormonal phases
…is empowering and reduces self-blame.
AI can help translate your data into simple summaries:
• “You often log low mood around days 24–28.”
• “You report joint pain more frequently in the luteal phase.”
That’s not a diagnosis, but it’s a conversation starter.
What AI Trackers Are Not (Especially for Irregular Cycles)
You should not rely on standard period apps for:
1. Contraception decisions
• Unless you are using a regulated, certified contraceptive app that specifically includes temperature/hormone data and has clear failure rates published, do not treat a generic “fertile window” as birth control.
2. Diagnosing PCOS, endometriosis, PMDD or other conditions
• Apps can flag “possible patterns,” but a diagnosis requires proper medical history, exam and sometimes imaging or lab tests.
3. Guaranteeing ovulation timing if you’re trying to conceive
• If TTC with irregular cycles, you’ll almost always need additional tools: LH strips, blood tests, scans or specialist input — not just app predictions.
4. Ruling out pregnancy or miscarriage
• “Your period is late” + “App says your cycle is now X days” ≠ safe reassurance. If in doubt, test and/or see a doctor.
AI doesn’t change these boundaries. It just makes the app more confident-sounding.
How to Use AI Period & Symptom Trackers Safely (Especially With PCOS/Endo)
1. Treat Predictions as Hypotheses, Not Instructions
Mentally downgrade all predictions:
• From: “My app says I’ll ovulate on Tuesday.”
• To: “Based on previous data, there’s a chance I might ovulate around Tuesday — but my body gets the final say.”
If you notice a big mismatch between the app and your real-world experience, believe your body.
2. Add Objective Data Where Possible
If you can, consider layering:
• Ovulation predictor kits (OPKs / LH strips)
• Basal body temperature (BBT) tracking
• Blood tests or ultrasounds ordered by a doctor
Into your tracking, so the app isn’t purely guessing based on calendar days.
Many apps let you log LH tests and BBT; some use this to refine predictions. It’s still not perfect, but it’s better than dates alone.
3. Log More Than Just Bleeding
For complex conditions, log:
• Pain (location + severity)
• Bowel/bladder symptoms
• Mood and energy
• Sleep
• Medications
• Major life events (stress spikes, travel, illness)
You’re building a longitudinal dataset about yourself that can help your future appointments, even if the app’s predictions are mediocre.
4. Bring Screenshots to Appointments
Instead of saying:
“My periods are all over the place.”
You can show:
• A 6–12-month graph of cycle lengths
• Symptom heatmaps
• Clusters of severe pain days
This shifts the conversation from “it’s probably just normal variation” to “here are the actual patterns.”
A good clinician will take this seriously.
Red Flags in AI Period & Symptom Trackers
Be wary if your app:
• Makes strong medical claims without clear disclaimers (e.g. “we can detect endometriosis from your tracking alone” — this is not currently evidence-based).
• Encourages you to skip contraception or frames itself as “natural birth control” without being certified as a contraceptive device with published effectiveness data.
• Dismisses irregularity as your fault, e.g. blaming you for “inconsistent logging” when your cycles are genuinely erratic.
• Pushes products or supplements aggressively based on your logged symptoms, especially if those products are from the same company.
• Doesn’t explain its limits — any honest app should be upfront that predictions are less accurate in PCOS/irregular cycles and not a substitute for medical care.
If in doubt, assume marketing is overselling and use the app conservatively.
How Sistapedia Fits In: From Generic Data to Reproductive-Health-First AI
Most mainstream apps were built for a general population, not specifically for complex reproductive health.
Sistapedia® is different by design.
We’re building the world’s first AI-verified marketplace and social platform dedicated solely to women’s reproductive health, across:
• PCOS, endometriosis and chronic pelvic pain
• Fertility, IVF, egg freezing, donor conception & surrogacy
• Pregnancy, birth, postpartum and breastfeeding
• Perimenopause, menopause and hormone health
The goal is not to hand you another “perfect period app.” It’s to:
• Combine AI tools with Crown Verified experts and Pink Tick Sistas
• Keep predictions clearly labelled as “guidance,” not diagnosis
• Use your tracking data to support better consults, not replace them
For Sistas
On Sistapedia, you will be able to:
• Log your cycles and symptoms in a space that understands PCOS, endo and irregularity as normal realities, not software bugs
• Get AI-assisted summaries that help you talk to your doctor more clearly
• See content and Q&As tailored to your condition, not generic 28-day cycle advice
💖 As you share your lived experience and support other women, you can apply for a free Pink Tick — our verification for Sistas who are helping build a smarter, safer reproductive health ecosystem.
For Experts & Femtech Founders
If you’re a:
• Gynaecologist, reproductive endocrinologist or GP
• Endometriosis / PCOS specialist, pelvic physio, psychologist, dietitian
• Femtech founder building responsible tracking tools
…Sistapedia is where you can:
• Create a professional profile and share how you use tracking data in real-world care
• Apply for Crown Verification so women know your expertise has been checked
• Connect with Sistas and product teams working to build next-generation AI tools that don’t erase complex cycles
👑 Crown Verification signals that you’re part of an ecosystem where AI is used with clinical judgement and lived experience — not instead of it.
Final Thoughts: Use the App, Don’t Worship It
AI period and symptom trackers can be:
• Helpful logs
• Decent pattern spotters
• Useful educational tools
They are not:
• A fertility crystal ball
• A contraceptive method on their own
• A way to self-diagnose (or rule out) serious conditions
If you have PCOS, endometriosis, chaotic cycles or you’re just getting the sense that your app’s confidence doesn’t match your reality, believe your body.
You’re allowed to say:
“This is interesting data — but I need a real conversation with a real specialist.”
✨ When you’re ready, join the sisterhood, and step into a space where your tracked data, your story and expert care actually talk to each other.