Month: June 2026
Placenta Health: The Organ That Sustains Pregnancy

When most people think about pregnancy, they think about the baby.
Few think about the organ that makes pregnancy possible.
The placenta.
It develops only during pregnancy.
It nourishes your baby.
Supplies oxygen.
Removes waste.
Produces hormones.
Protects against many infections.
Coordinates communication between mother and baby.
Then, after birth, it has completed its purpose.
Despite being one of the most important organs in pregnancy, the placenta is rarely discussed outside the delivery room.
Yet placental health influences almost every aspect of pregnancy—from fetal growth and development to the timing of birth.
Understanding how the placenta works helps women better understand their pregnancy and why routine antenatal care is so important.
Quick Answer
The placenta is a temporary organ that develops during pregnancy to supply oxygen, nutrients, hormones and immune support to the growing baby. A healthy placenta is essential for normal fetal growth and development, while problems affecting placental function may increase the risk of pregnancy complications.
What Is the Placenta?
The placenta begins forming shortly after a fertilised embryo implants into the uterus.
Over the following weeks it develops into an extraordinary organ that connects mother and baby through the umbilical cord.
Although their circulatory systems remain separate, the placenta allows an exchange of:
- oxygen
- nutrients
- antibodies
- hormones
- waste products
This exchange supports every stage of fetal development.
Without a functioning placenta, pregnancy cannot continue.
Why Is the Placenta So Important?
Many people think the placenta simply “feeds the baby.”
Its role is far greater.
The placenta functions as:
- the baby’s lungs
- the baby’s kidneys
- the baby’s digestive support system
- a hormone-producing organ
- an immune interface between mother and baby
Few organs in medicine perform so many functions simultaneously.
How Does the Placenta Feed the Baby?
Everything the developing baby needs must first pass through the placenta.
This includes:
- oxygen
- glucose
- amino acids
- fatty acids
- vitamins
- minerals
The placenta carefully regulates this transfer.
It is not simply a passive filter.
It actively transports many nutrients while helping remove carbon dioxide and metabolic waste from the baby’s circulation.
Does the Placenta Produce Hormones?
Yes.
In fact, the placenta becomes one of the body’s most active hormone-producing organs during pregnancy.
It produces hormones including:
- human chorionic gonadotropin (hCG)
- progesterone
- estrogen
- human placental lactogen (hPL)
These hormones help:
- maintain pregnancy
- support fetal growth
- prepare the breasts for breastfeeding
- influence maternal metabolism
The placenta acts as both a life-support system and an endocrine organ.
What Most Women Are Not Told #1
Many pregnancy symptoms that women experience—including nausea, fatigue, breast tenderness and changing metabolism—are influenced not only by the baby, but by hormones produced by the placenta itself.
What Can Affect Placental Health?
Most placentas develop normally.
However, some pregnancies experience placental complications.
These may include:
- reduced blood flow
- abnormal implantation
- placental insufficiency
- placental abruption
- placenta previa
The severity varies considerably between pregnancies.
Many placental conditions are identified through routine antenatal monitoring before they become emergencies.
Looking for trusted information across fertility, pregnancy, birth, postpartum recovery and women’s health?
Explore hundreds of evidence-based articles on Sistapedia, written to help women make informed health decisions at every stage of life.
How Does Placental Health Affect Baby’s Growth?
As pregnancy progresses, the baby’s nutritional needs increase dramatically.
If the placenta is unable to supply sufficient oxygen or nutrients, fetal growth may slow.
Healthcare providers monitor this through:
- ultrasound assessments
- fetal growth measurements
- Doppler blood flow studies
- maternal health assessments
The purpose of monitoring is early detection and timely intervention.
Can Lifestyle Influence Placental Health?
Some factors are beyond anyone’s control.
Others support a healthy pregnancy overall.
General recommendations include:
- attending regular antenatal appointments
- managing chronic medical conditions
- avoiding smoking
- limiting alcohol exposure
- maintaining appropriate nutrition
- following medical advice throughout pregnancy
Healthy pregnancy care supports both maternal and placental health.
Why Is the Placenta Called the “Forgotten Organ”?
After birth, attention naturally shifts to the baby.
The placenta is delivered and often discarded.
Yet throughout pregnancy it has sustained two lives simultaneously.
Researchers continue discovering new roles for the placenta in:
- fetal programming
- maternal health
- immune regulation
- long-term child development
It remains one of the least appreciated organs in medicine.
What Most Women Are Not Told #2
The placenta records much of the pregnancy.
Healthcare professionals may examine it after birth because it can provide important clues about complications affecting both mother and baby.
What Happens After the Baby Is Born?
Once the baby is delivered, the uterus contracts and the placenta separates from the uterine wall.
This stage is known as the third stage of labour.
Healthcare providers examine the placenta to ensure it has been delivered completely.
Retained placental tissue can increase the risk of:
- heavy bleeding
- infection
- delayed postpartum recovery
Can Placental Problems Be Prevented?
Not all placental complications can be prevented.
Many occur despite excellent prenatal care.
However, early antenatal care improves the likelihood that problems are recognised promptly and managed appropriately.
Modern obstetrics has significantly improved outcomes through earlier monitoring and better understanding of placental disease.
What Most Women Are Not Told #3
The placenta does not simply support pregnancy.
It actively influences how the baby’s organs develop before birth.
Scientists increasingly believe placental function may affect health long after delivery, making it one of the most important organs in lifelong human development.
Frequently Asked Questions
Does every pregnancy develop a placenta?
Yes. A functioning placenta is essential for an ongoing pregnancy.
Can the placenta repair itself?
Some placental changes may compensate over time, but significant placental disease requires medical monitoring.
Is an anterior placenta dangerous?
Usually not. An anterior placenta refers to its position and is often a normal variation.
Why do doctors monitor the placenta during pregnancy?
Because placental function directly influences fetal growth, oxygen supply and pregnancy outcomes.
The Bigger Picture
The placenta is one of the most extraordinary organs the human body ever produces.
It exists for only one pregnancy.
Yet during those months it performs the work of multiple organs while supporting the growth of an entirely new life.
Understanding placental health helps women better understand pregnancy itself.
And informed women are better equipped to recognise the importance of routine antenatal care, ongoing monitoring and asking questions throughout their pregnancy journey.
Secure Your Position Now
Verified Sista’s receive a free Pink Tick, signalling genuine, trusted identity across Sistapedia.
Women come to Sistapedia®️ to learn. Professionals come to educate.
If you’re a Medical Doctor, Registered Nurse, Healthcare Practitioner, Expert, Product or Brand in women’s health, visit the Verification tab in your profile and apply for Crown Verification.
Start publishing content, join our global directories, and secure your position among the trusted voices shaping women’s health.
Select the Verification tab in your profile to get started.
Coping with Life
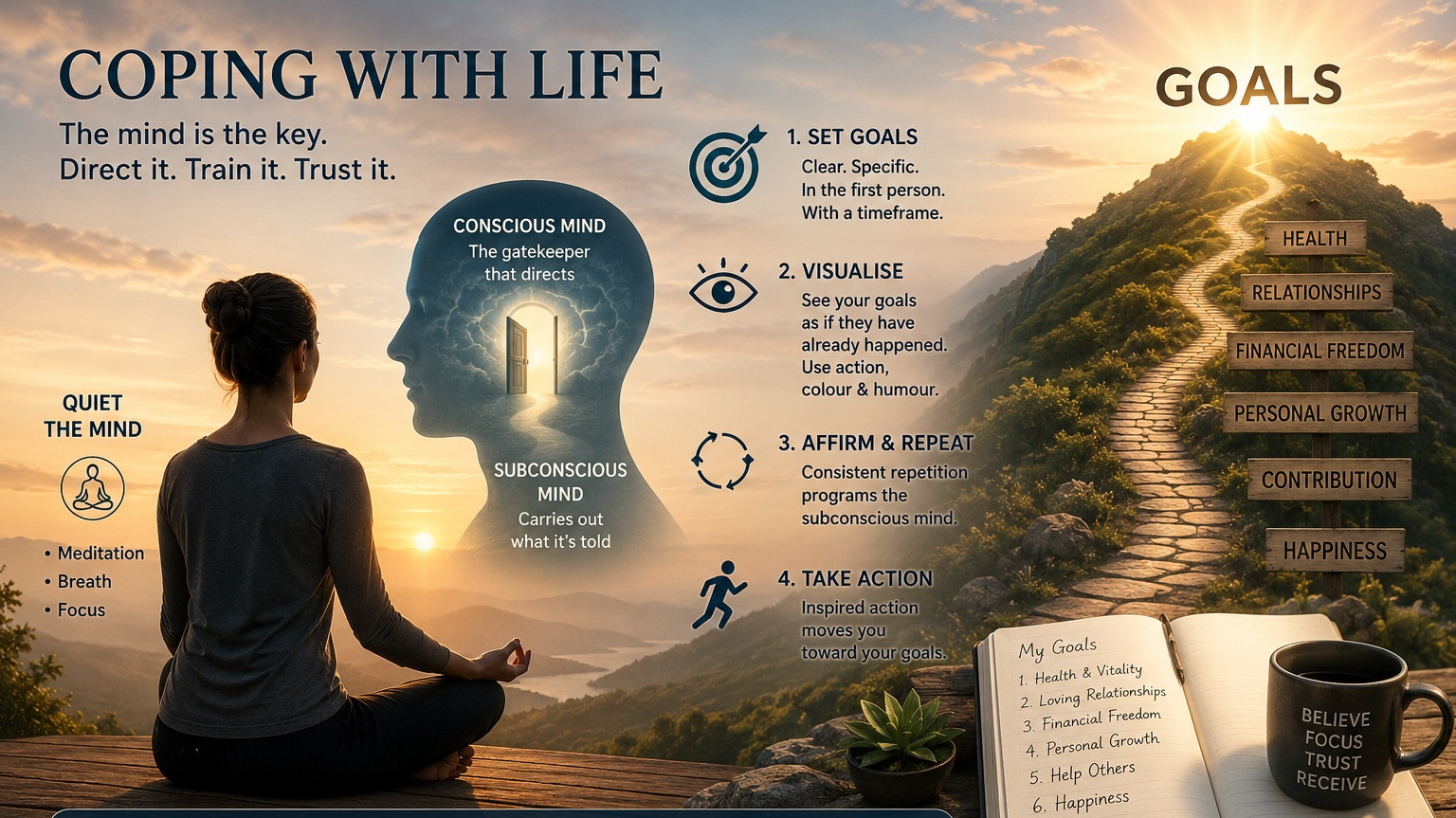
Coping with Life
I recently wrote an article, ‘Coping with Technology’ and what struck me was the similarity with the human mind and how we cope with our everyday life. So here is a brief overview of my own strategies, which have been quite successful.
Firstly, this is about the mind. Our mind is where it all happens, and so those people who are successful are those who know how to use their mind. In the previous article we had to be very precise with how we tasked our AI with well written unambiguous Prompts. The good news is that the mind is no different and needs precise directions with no wiggle room.
I was fortunate that in one of my earlier jobs, the company sent me on a personal development course, ‘Investment in Excellence’. The central theme was the development of Goals, basically the equivalent of an AI Prompt. I cannot overstate the effectiveness of Goals; they need to be first person, specific, and have a time frame; you can have many Goals covering, both your personal and business life.
My wife and I have worked in ten-year time frames, agreed on our Goals, affirmed the Goals regularly for a couple of months to make sure the subconscious part of our mind has got the message, then put them away. Generally, in winter relaxed around the fire, about ten years later we have opened the draw and reviewed our goals, to find without exception all Goals have been achieved! We have done this for decades with the same result. Once a Goal is achieved you need a new Goal or you become complacent; so, the trick is to generate a new set of Goals and maintain the movement; otherwise, you lose energy.
Well, that is the big picture; how does the mind now make it happen, this is the hard part. This is now about training the mind. We need a still and quiet mind, not a monkey brain buzzing away undirected. Meditation is the first step, learning to quieten the mind and develop the ability to focus your mind; this is not easy and takes time; belly or diaphragm breathing is a key ingredient to total relaxation and focus; taking belly breathes is not normal but easily learned. Once you have mastered this technique, the next step is visualisation while in a meditative state. In this technique you visualise your goals as if they have already occurred. Your subconscious knows no better and moves you in this direction assuming it has already happened.
A brief note here; the mind has two parts; the conscious and subconscious part. The conscious part is the gate that directs the subconscious; the subconscious only knows what the conscious mind tells it. So, you tell it what you want and this gets the train moving in the right direction. A word of caution: the subconscious does not know the difference between good and bad thoughts, so be careful of what you think, it can go the wrong way.
A useful trick is to use a key word as part of your relaxation / meditation training; you say the key word and your subconscious gets directed by your conscious mind to relax.
So, once you have set your Goals, go into a meditative state and visualise each of your Goals as if it has already occurred; action, colour and humour make this process more effective; repeat this process many times, over a period of weeks / months and the results can be truly mind blowing.
Well, that’s the process and it works!
It is not easy, but gets easier with training. There is a lot of material out there on this topic, but the basic principles are as I have described. You cannot be a spectator in this process and it is essential you believe; remember the subconscious believes what you tell it.
Over many years I have studied many books on this subject and the standout reference is ‘The Master Key System’, by Charles Haanel; this a book by someone who knew his craft and practiced it.
Why Ovulation Timing Is More Complex Than Most Apps Suggest

For women trying to conceive, few dates feel more important than ovulation day.
Countless apps promise to predict it.
Calendars estimate it.
Algorithms forecast it.
Notifications remind women when their “fertile window” begins.
But there is one problem.
The female body does not always follow the calendar.
While ovulation tracking technology has improved dramatically, ovulation itself remains a biological process influenced by hormones, stress, sleep, illness, age, and countless individual factors.
For some women, ovulation occurs exactly when predicted.
For many others, it does not.
Understanding this distinction is important because fertility timing remains one of the most misunderstood aspects of reproductive health.
Ovulation is the release of an egg from the ovary, typically occurring once during a menstrual cycle. While apps estimate ovulation using cycle data, actual ovulation can vary significantly between cycles. Hormones, stress, illness, age, sleep, and underlying conditions such as PCOS can all affect timing.
What Is Ovulation?
Ovulation occurs when a mature egg is released from the ovary.
After release:
- the egg travels into the fallopian tube
- fertilisation may occur
- the egg survives approximately 12–24 hours
Because the egg’s lifespan is short, timing matters.
However, fertility is not limited to a single day.
What Is the Fertile Window?
The fertile window refers to the days during which pregnancy is most likely to occur.
This includes:
- the days before ovulation
- ovulation day itself
Sperm can survive within the female reproductive tract for several days.
This means pregnancy can occur even if intercourse happens before ovulation.
Why Do Ovulation Apps Sometimes Get It Wrong?
Most apps estimate ovulation using previous cycle lengths.
This approach assumes:
- cycles are consistent
- ovulation occurs predictably
- biology follows averages
Many women’s bodies do not behave this way.
Cycle length and ovulation timing can shift naturally.
An app cannot directly see ovulation.
It is making an educated prediction.
What Most Women Are Not Told #1
A regular period does not automatically guarantee ovulation occurred.
Some women experience menstrual bleeding without releasing an egg.
This is one reason fertility challenges sometimes surprise women with apparently normal cycles.
Can Stress Delay Ovulation?
Yes.
The reproductive system is closely connected to the brain.
Stress can influence:
- hormone production
- ovulation timing
- cycle length
This does not mean every stressful week prevents pregnancy.
However, significant physical or emotional stress can alter reproductive patterns.
How Does Age Affect Ovulation?
As women age:
- ovarian reserve declines
- egg quality declines
- hormonal patterns become less predictable
Cycles often become more variable during the late reproductive years and perimenopause.
This variability can make ovulation prediction more challenging.
Looking for trusted information across fertility, pregnancy, postpartum recovery, newborn health, breastfeeding, menopause, and reproductive medicine?
Explore hundreds of evidence-based articles on Sistapedia.
What About PCOS?
Polycystic Ovary Syndrome (PCOS) is one of the most common causes of ovulation disruption.
Women with PCOS may experience:
- irregular cycles
- delayed ovulation
- infrequent ovulation
- absent ovulation
For these women, calendar-based prediction methods are often less reliable.
What Most Women Are Not Told #2
The “day 14 ovulation” rule is a population average.
Many healthy women ovulate earlier.
Many healthy women ovulate later.
There is no universal ovulation day.
How Can Women Better Understand Ovulation?
Many women combine multiple indicators including:
- cycle tracking
- cervical mucus changes
- ovulation predictor kits
- basal body temperature
Each provides different information.
No single method is perfect.
Together, they often provide a more complete picture.
Why Fertility Is More Than Timing
Timing matters.
But fertility also depends on:
- egg quality
- sperm quality
- tubal function
- uterine health
- hormonal balance
Ovulation is only one piece of a much larger reproductive system.
What Most Women Are Not Told #3
Many couples assume conception should occur immediately once ovulation is identified.
In reality, even healthy couples have a limited chance of conception each cycle.
Pregnancy is a biological probability—not a guarantee.
Frequently Asked Questions
Can you get pregnant outside your fertile window?
It is less likely, but cycle variability means exact fertile windows are not always obvious.
Do all women ovulate every month?
No. Some cycles may occur without ovulation.
Are ovulation apps accurate?
They can be helpful guides, but they predict rather than directly measure ovulation.
Does irregular ovulation mean infertility?
No. Many causes of irregular ovulation are treatable.
The Bigger Picture
Technology has made fertility tracking more accessible than ever.
But reproductive biology remains more complex than a smartphone notification.
Understanding ovulation means understanding variability.
The goal is not perfect prediction.
The goal is understanding how your body works.
That knowledge creates better decisions, better conversations, and often less anxiety throughout the fertility journey.
Secure Your Position Now
Verified Sista’s receive a free Pink Tick, signalling genuine, trusted identity across Sistapedia®️.
Women come to Sistapedia®️ to learn. Professionals come to educate.
If you’re a Medical Doctor, Registered Nurse, Healthcare Practitioner, Expert, Product or Brand in women’s health, visit the Verification tab in your profile and apply for Crown Verification.
Start publishing content, join our global directories, and secure your position among the trusted voices shaping women’s health.
Select the Verification tab in your profile to get started.
How Infant Gut Development Shapes Early Health

When parents think about newborn health, they often focus on the obvious milestones.
Sleeping.
Feeding.
Growth.
Development.
But one of the most important systems influencing a baby’s future health cannot be seen.
The gut.
Inside a newborn’s digestive system, trillions of microorganisms begin establishing what scientists call the gut microbiome—a complex ecosystem of bacteria, viruses, fungi, and other microbes.
Far from being harmful, many of these microorganisms play essential roles in health.
They help train the immune system.
Support digestion.
Protect against harmful pathogens.
And influence health outcomes long after infancy.
Researchers increasingly believe that some of the foundations for lifelong health are established during the earliest months and years of life.
Understanding infant gut development is becoming one of the most important areas of modern pediatric and reproductive health research.
Infant gut development refers to the formation and maturation of the digestive microbiome during early life. The infant gut helps shape immune function, digestion, metabolism, and protection against disease. Factors such as birth method, feeding choices, antibiotic exposure, and environment can influence how the gut microbiome develops.
What Is the Infant Gut Microbiome?
The gut microbiome is the collection of microorganisms that live within the digestive tract.
Adults carry trillions of microbes.
Newborns begin life with a microbiome that is still developing.
During infancy, the gut becomes populated by a diverse community of microorganisms that interact continuously with:
- the digestive system
- the immune system
- metabolic pathways
- the nervous system
This process is dynamic and changes rapidly during the first years of life.
Why Is Gut Development So Important?
The gut is often viewed purely as a digestive organ.
But it performs far broader functions.
The infant gut plays a role in:
- nutrient absorption
- immune development
- infection protection
- inflammatory regulation
- metabolic programming
Some researchers estimate that approximately 70% of immune system activity is connected to the gastrointestinal tract.
This makes early gut development particularly important.
How Does a Baby’s Gut Develop After Birth?
A newborn’s gut is not fully mature at birth.
Development continues rapidly throughout infancy.
The microbiome evolves through:
Early microbial exposure
Microorganisms begin colonizing the infant gut shortly after birth.
Feeding
Breast milk, formula, and later solid foods all influence microbial diversity.
Environmental exposure
Family members, pets, siblings, and surroundings contribute microbial exposure.
Immune maturation
The developing immune system learns to distinguish beneficial microbes from harmful pathogens.
These processes work together to build a more complex and resilient microbiome.
Does Birth Method Influence Gut Development?
Research suggests birth method may influence early microbial exposure.
Babies born vaginally encounter microorganisms from the birth canal during delivery.
Babies born via cesarean section may experience different early microbial patterns.
However, birth method is only one factor.
The microbiome continues evolving after birth through feeding, environment, and ongoing exposures.
What Most Parents Are Not Told #1
Birth method does not determine a baby’s future health destiny.
While microbial differences may exist initially, many factors influence gut development during infancy.
The microbiome continues changing long after delivery.
Why Is Breast Milk Important for Gut Health?
Breast milk contains more than nutrition.
It also contains:
- antibodies
- immune factors
- beneficial compounds
- human milk oligosaccharides (HMOs)
HMOs are unique carbohydrates that nourish beneficial gut bacteria.
Interestingly, babies do not digest HMOs directly.
Instead, these compounds feed specific microorganisms that help establish a healthy microbiome.
This is one reason breast milk is considered biologically sophisticated.
What About Formula-Fed Babies?
Formula-fed babies also develop microbiomes.
The microbial composition may differ somewhat from exclusively breastfed infants, but gut development continues regardless of feeding pathway.
Modern infant nutrition has evolved significantly.
The goal should never be guilt.
The goal should be supporting infant health using the feeding approach that is safest, most sustainable, and most appropriate for each family.
Looking for trusted information across fertility, pregnancy, postpartum recovery, newborn health, breastfeeding, menopause, and reproductive medicine?
Explore hundreds of evidence-based articles on Sistapedia.
How Does the Gut Influence the Immune System?
One of the most important jobs of the infant microbiome is immune education.
The immune system must learn:
- what is dangerous
- what is harmless
- what should be tolerated
Beneficial gut bacteria help guide these processes.
Researchers continue studying how early microbial development may influence future risks for:
- allergies
- eczema
- asthma
- autoimmune disease
The science continues evolving, but the connection between gut development and immune health is now widely recognized.
Can Antibiotics Affect Infant Gut Development?
Antibiotics save lives and remain one of the most important tools in modern medicine.
However, antibiotics do not distinguish between harmful and beneficial bacteria.
This means antibiotic exposure may temporarily alter the microbiome.
Healthcare decisions should always balance:
- benefits
- risks
- clinical necessity
When antibiotics are needed, appropriate treatment remains the priority.
What Most Parents Are Not Told #2
The goal is not to avoid every microbial disruption.
The goal is resilience.
Healthy microbiomes are dynamic and adaptable.
Temporary changes do not automatically lead to long-term problems.
What Happens When Babies Start Solid Foods?
The introduction of solids represents a major developmental milestone for the microbiome.
New foods introduce:
- new nutrients
- new fibers
- new microbial influences
As dietary diversity increases, microbial diversity often increases as well.
This transition helps the gut move toward a more mature state.
Is There a Connection Between the Gut and the Brain?
Researchers increasingly study what is known as the gut-brain axis.
This refers to communication between:
- the digestive system
- the nervous system
- the brain
While infant research is still developing, scientists believe gut health may influence:
- behavior
- mood
- neurological development
- immune regulation
This area remains one of the most exciting fields in modern health research.
What Most Parents Are Not Told #3
Many aspects of infant health are interconnected.
The gut influences immunity.
Immunity influences inflammation.
Inflammation influences development.
Health systems do not operate independently.
The microbiome is part of a much larger biological network.
Can Parents Support Healthy Gut Development?
No parent can create a “perfect” microbiome.
And perfection is not the goal.
However, healthy development is supported through:
- appropriate infant nutrition
- routine healthcare
- safe environmental exposure
- responsive caregiving
- evidence-based medical care
Small, consistent factors often matter more than individual interventions.
Frequently Asked Questions
Does every baby have a microbiome?
Yes. All babies develop microbiomes, although microbial composition differs between individuals.
Can gut health affect immunity?
Yes. The gut plays a major role in immune system development.
Is breastfeeding required for healthy gut development?
No. Breastfeeding provides unique biological benefits, but healthy development can occur through multiple feeding pathways.
Does the microbiome stop changing after infancy?
No. The microbiome continues evolving throughout life.
The Bigger Picture
The infant gut is far more than a digestive system.
It is one of the body’s earliest training grounds.
The microbiome helps shape:
- digestion
- immunity
- metabolism
- health resilience
Scientists continue discovering how profoundly these early years influence future wellbeing.
While no parent can control every variable, understanding the importance of gut development provides valuable insight into one of the most remarkable systems in human biology.
Secure Your Position Early
Verified Sista’s receive a free Pink Tick, signalling genuine, trusted identity across Sistapedia.
Women come to Sistapedia to learn. Professionals come to educate.
If you’re a Medical Doctor, Registered Nurse, Healthcare Practitioner, Expert, Product or Brand in women’s health, visit the Verification tab in your profile and apply for Crown Verification.
Start publishing content, join our global directories, and secure your position among the trusted voices shaping women’s health.
Select the Verification tab in your profile to get started.
Why Endometriosis Takes Years to Diagnose: The Hidden Cost of Women’s Pain

For many women, endometriosis begins with a sentence they hear repeatedly:
“Painful periods are normal.”
So they push through.
They go to school in pain.
They work in pain.
They parent in pain.
They exercise in pain.
They have sex in pain.
And often, they do this for years before receiving a diagnosis.
Endometriosis affects an estimated 1 in 9 women in Australia and millions worldwide. Yet despite its prevalence, diagnosis frequently takes many years.
The result is not only physical suffering, but also lost productivity, fertility challenges, relationship strain, and significant impacts on mental health.
Endometriosis is far more than “bad periods.”
It is a chronic inflammatory disease.
And for many women, the pain extends well beyond menstruation
Quick Answer
Endometriosis occurs when tissue similar to the lining of the uterus grows outside the uterus. These lesions can trigger inflammation, scarring, and chronic pain. Diagnosis often takes years because symptoms vary widely, overlap with other conditions, and menstrual pain is frequently normalized.
What Is Endometriosis?
Endometriosis occurs when tissue resembling the endometrium grows outside the uterus.
These growths may be found on:
- ovaries
- fallopian tubes
- pelvic lining
- bowel
- bladder
- ligaments
- diaphragm
Each month, these tissues respond to hormonal changes.
Unlike menstrual blood leaving the body, these lesions can trigger:
- inflammation
- irritation
- scar formation
- adhesions
Over time, chronic inflammation may contribute to ongoing pain.
Why Does Endometriosis Cause So Much Pain?
Pain in endometriosis is complex.
It is not simply about the amount of tissue present.
Some women with extensive disease have few symptoms.
Others with minimal disease experience severe pain.
Pain may arise from:
- inflammation
- nerve involvement
- adhesions
- muscle dysfunction
- central nervous system sensitization
This helps explain why symptoms vary dramatically between women.
What Does Endometriosis Pain Feel Like?
Symptoms differ from person to person.
Women may experience:
- severe menstrual cramps
- chronic pelvic pain
- lower back pain
- painful ovulation
- painful intercourse
- bowel pain
- painful urination
- bloating
- fatigue
Some women describe the pain as:
- stabbing
- burning
- pulling
- cramping
- radiating
Importantly, symptoms can occur throughout the month—not only during periods.
Why Does Diagnosis Take So Long?
Historically, endometriosis has been under-recognized.
Symptoms often overlap with:
- irritable bowel syndrome (IBS)
- bladder disorders
- musculoskeletal pain
- gastrointestinal conditions
Many women are also told:
- “Periods are supposed to hurt.”
- “You’ll grow out of it.”
- “Pregnancy will fix it.”
- “It’s just stress.”
These messages can delay investigation.
What Most Women Are Not Told #1
Severe period pain that interferes with school, work, or daily activities is not considered normal.
Pain significant enough to regularly disrupt life deserves medical assessment.
Can Endometriosis Affect Fertility?
Yes.
Endometriosis may affect fertility through several mechanisms:
- inflammation
- altered pelvic anatomy
- scarring
- reduced egg quality
- impaired implantation
However, many women with endometriosis do conceive naturally.
A diagnosis does not automatically mean infertility.
Fertility outcomes vary widely between individuals.
Why Do Some Women Experience Pain Even After Surgery?
Surgery can be life-changing for some women.
But for others, pain persists.
This occurs because chronic pain is not always driven solely by visible lesions.
Long-term pain can affect the nervous system itself.
Over time, the brain and spinal cord may become more sensitive to pain signals—a process known as central sensitization.
This means pain may continue even after lesions are removed.
Looking for trusted women’s health information?
Join Sistapedia to access evidence-based articles, expert insights, and verified voices across fertility, pregnancy, postpartum recovery, hormonal health, menopause, and reproductive medicine.
Is Endometriosis Only a Reproductive Disease?
No.
Endometriosis affects far more than reproduction.
Women commonly report impacts on:
- education
- careers
- relationships
- exercise
- sleep
- mental health
Research increasingly recognizes endometriosis as a whole-body inflammatory condition with broad health implications.
What Most Women Are Not Told #2
Endometriosis symptoms do not always correlate with disease severity.
A woman experiencing severe pain may have relatively small lesions, while another with extensive disease may have few symptoms.
Pain is real regardless of disease stage.
Can Endometriosis Affect Mental Health?
Living with chronic pain can significantly affect emotional wellbeing.
Women with endometriosis may experience:
- anxiety
- depression
- social isolation
- reduced quality of life
This does not mean the pain is psychological.
It means chronic physical symptoms affect mental health—as they would with any long-term illness.
Both deserve care.
How Is Endometriosis Diagnosed?
Diagnosis may involve:
- medical history
- pelvic examination
- ultrasound
- MRI
- specialist review
Historically, surgery was considered the gold standard for diagnosis.
Today, imaging and clinical assessment increasingly contribute to earlier recognition.
However, diagnosis remains challenging.
Is There a Cure for Endometriosis?
Currently, there is no known cure.
Management depends on:
- symptom severity
- fertility goals
- age
- personal preferences
Treatment approaches may include:
- pain management
- hormonal therapy
- surgery
- physiotherapy
- lifestyle strategies
- fertility treatment where appropriate
Management is individualized.
No single treatment works for every woman.
What Most Women Are Not Told #3
Endometriosis is often invisible.
Many women look healthy while living with significant pain every day.
Invisible illness can make it harder for others to understand the impact.
That does not make the symptoms any less real.
When Should You Seek Medical Advice?
Medical review should be considered if you experience:
- severe menstrual pain
- pain during sex
- chronic pelvic pain
- fertility difficulties
- symptoms affecting daily life
Earlier recognition may improve symptom management and reproductive outcomes.
Frequently Asked Questions
Can endometriosis get worse with age?
Symptoms may change over time, although progression varies between individuals.
Does pregnancy cure endometriosis?
No. Symptoms may temporarily improve for some women, but pregnancy is not considered a cure.
Can teenagers develop endometriosis?
Yes. Symptoms may begin during adolescence.
Can endometriosis return after surgery?
Yes. Recurrence can occur in some women.
The Bigger Picture
Endometriosis is one of the most common—and most misunderstood—women’s health conditions.
For too long, women have been told their pain is normal.
It is not.
Pain that disrupts education, work, relationships, or quality of life deserves investigation.
Earlier recognition leads to earlier support.
And women deserve both.
Secure your position early.
Verified Sista’s receive a free Pink Tick, signalling genuine, trusted identity across Sistapedia.
Women come to Sistapedia to learn. Professionals come to educate.
If you’re a Medical Doctor, Registered Nurse, Healthcare Practitioner, Expert, Product or Brand in women’s health, visit the Verification tab in your profile and apply for Crown Verification.
Start publishing content, join our global directories, and secure your position among the trusted voices shaping women’s health.
Select the Verification tab in your profile to get started.
Secondary Infertility: Why Getting Pregnant Again Can Be Harder the Second Time

For many couples, the first pregnancy creates an assumption.
If it happened once, it should happen again.
Perhaps not immediately.
Perhaps not on the first attempt.
But eventually.
When months pass without success, confusion often follows.
After all, fertility problems happen to other people.
Not couples who have already had a child.
Yet secondary infertility is surprisingly common.
In fact, many women are completely unprepared for the emotional shock that comes with struggling to conceive after previously becoming pregnant naturally or successfully having a child.
The challenge is not just fertility itself.
It is the expectation that fertility should still work exactly as it did before.
And biology does not always cooperate with expectations.
Secondary infertility is the inability to conceive or carry a pregnancy to term after previously having a child. It can result from age-related fertility decline, reduced egg quality, ovulation disorders, sperm changes, endometriosis, miscarriage, lifestyle factors, or unexplained fertility issues. Many of the same causes that affect primary infertility can also affect fertility after a successful pregnancy.
What Is Secondary Infertility?
Secondary infertility occurs when:
- a couple has previously conceived or had a child
- but is unable to conceive again despite regular unprotected intercourse
The diagnosis criteria are generally similar to primary infertility:
- under 35 years old: 12 months of trying
- over 35 years old: 6 months of trying
The difference is psychological.
With primary infertility, there is uncertainty about whether conception is possible.
With secondary infertility, there is often disbelief that fertility has changed at all.
Why Does Secondary Infertility Surprise So Many Women?
Because fertility is often viewed as a permanent capability.
Many people think:
“I got pregnant before, so I know everything works.”
But fertility is not fixed.
It changes continuously throughout life.
Age changes it.
Health changes it.
Hormones change it.
Sperm changes.
Egg quality changes.
Reproductive health conditions can develop years after a first pregnancy.
The body that conceived at 29 is not necessarily the same body attempting conception at 35, 38, or 42.
Why can fertility decline after having a child?
This is one of the most common questions fertility specialists hear.
Many women assume pregnancy somehow “proves” future fertility.
It doesn’t.
Pregnancy proves fertility existed at a specific moment in time.
It does not guarantee future fertility.
Several biological changes may occur between pregnancies:
- declining ovarian reserve
- reduced egg quality
- sperm quality changes
- weight changes
- hormonal changes
- reproductive health conditions
- increased chronic stress
Fertility is dynamic.
Not static.
What role does age play in secondary infertility?
Age remains one of the most significant factors.
Women are born with their lifetime supply of eggs.
Over time:
- egg quantity declines
- egg quality declines
The decline in egg quality becomes increasingly important after age 35.
This affects:
- fertilization rates
- embryo development
- miscarriage risk
- chromosomal abnormalities
What most women are not told
Many women understand that fertility declines with age.
Far fewer understand that egg quality often declines faster than egg quantity.
A woman may still have regular periods and still experience significant fertility decline.
Can sperm quality change between pregnancies?
Yes.
This is often overlooked.
Fertility conversations frequently focus on women.
But sperm quality changes over time as well.
Factors that may affect sperm include:
- age
- smoking
- alcohol
- obesity
- medications
- environmental exposures
- medical conditions
A couple may have conceived easily years earlier and now face fertility challenges due to changes affecting either partner.
Could endometriosis or PCOS develop after a first pregnancy?
Absolutely.
Some reproductive conditions are only diagnosed years later.
Endometriosis
Endometriosis can:
- worsen over time
- affect egg quality
- alter pelvic anatomy
- impair fertilization
PCOS
PCOS may affect:
- ovulation
- hormone regulation
- metabolic health
Some women only discover these conditions after struggling to conceive again.
Looking for real, verified information in women’s health?
Join Sistapedia and access trusted voices across every stage of the reproductive lifecycle.
What about miscarriage and pregnancy loss?
Not all fertility journeys end in successful pregnancy.
Some couples experiencing secondary infertility are actually experiencing:
- recurrent pregnancy loss
- chemical pregnancies
- failed implantation
Conception may be occurring.
The challenge may be maintaining the pregnancy.
This distinction is important because the investigations and treatment pathways can differ significantly.
Why does secondary infertility feel emotionally different?
Many women describe secondary infertility as uniquely isolating.
They often feel:
- guilty for wanting another child
- pressure not to complain because they already have a child
- misunderstood by family and friends
Comments such as:
“You already have one.”
or
“At least you know you can get pregnant.”
can feel dismissive.
The desire to grow a family is not reduced simply because a child already exists.
What most women are not told
Secondary infertility often carries a hidden grief.
Women are simultaneously:
- parenting a child
- grieving the family they imagined having
Both realities can exist at the same time.
When should you seek fertility testing?
Women should generally seek evaluation after:
- 12 months if under 35
- 6 months if over 35
Earlier assessment may be appropriate when there is:
- known endometriosis
- PCOS
- irregular cycles
- recurrent miscarriage
- previous fertility treatment
Earlier answers often create more options.
What tests are commonly performed?
Fertility investigations may include:
Ovarian reserve assessment
Often involving:
- AMH testing
- antral follicle count
Ovulation assessment
To determine whether ovulation is occurring regularly.
Tubal assessment
To assess whether fallopian tubes remain open.
Uterine assessment
To identify:
- fibroids
- polyps
- scarring
Semen analysis
To evaluate sperm health.
Can secondary infertility be unexplained?
Yes.
In some cases, testing reveals no obvious cause.
This is called unexplained infertility.
It can be frustrating because:
- fertility appears normal
- conception is not occurring
However, “unexplained” does not mean “untreatable.”
It simply means current testing has not identified a clear explanation.
What treatment options exist?
Treatment depends entirely on the underlying cause.
Options may include:
Lifestyle interventions
Addressing:
- weight
- nutrition
- sleep
- smoking
- alcohol
Ovulation induction
Used when ovulation is irregular.
IUI
Intrauterine insemination may be appropriate in some cases.
IVF
IVF may be recommended when:
- age is a major factor
- tubal issues exist
- severe male factor infertility exists
- previous treatments have failed
The correct pathway depends on the individual clinical picture.
What most women are not told
Many women assume fertility treatment begins with IVF.
It doesn’t.
The first step is understanding why conception is not occurring.
Without identifying the problem, it is difficult to choose the right solution.
Fertility treatment is not one treatment.
It is a series of possible interventions based on diagnosis.
Frequently Asked Questions
Is secondary infertility common?
Yes. It affects a significant number of families worldwide.
Can you get pregnant naturally after secondary infertility?
Yes. Some couples conceive naturally after evaluation or treatment.
Is age always the reason?
No. Age is important, but it is only one of many possible factors.
Does having a child prove fertility is still normal?
No. Fertility can change significantly between pregnancies.
Should men be tested too?
Yes. Male fertility factors contribute to many infertility cases.
The Bigger Picture
Secondary infertility challenges one of the most common assumptions in reproductive health:
that fertility remains unchanged simply because pregnancy happened before.
It doesn’t.
The reproductive system evolves throughout life.
Health changes.
Hormones change.
Eggs change.
Sperm changes.
Understanding this does not make the journey easier.
But it makes it more understandable.
And for many women, understanding what is happening is the first step toward finding the right path forward.
The future leaders in women’s health won’t arrive after the audience is built. They’ll already be there.
Verified Sista’s are identified with a free Pink Tick, helping women connect with genuine, trusted voices across women’s health.
Medical Doctors, Registered Nurses, Healthcare Practitioners, Experts, Products and Brands can establish an early presence through Professional Crown Verification and position themselves alongside a growing network of trusted participants across women’s reproductive health.
The women, professionals, products and brands that move early will be the most visible as awareness, participation and opportunity continue to grow.
Secure your position early. Hit the Apply for Verifycation tab in your profile – start posting content, and join our global directories for free.